Fig. 26.1
Pediatric/infant offset cystoscope
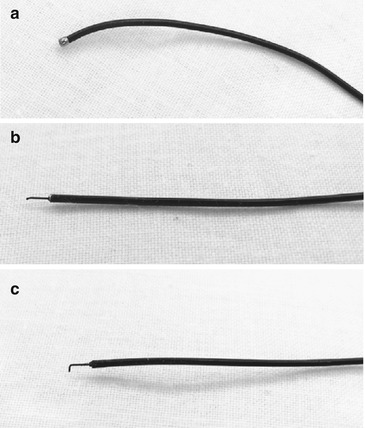
Fig. 26.2
A variety of probes are used for endoscopic treatment of ureteroceles and syringoceles. (a) Bugbee-type probe. (b) Needle-type probe. (c) Right-angle-type probe
Operative Technique
For infants and small children, a gel roll or towel roll underneath the legs is adequate to elevate the lower extremities in a lithotomy position. The legs will need to be secured to the table with tape to prevent any slippage. Accordingly, the skin will need protection with gauze or a small towel. Pediatric-size stirrups or candy canes may be used for toddlers and older children (Fig. 26.3). Lastly, it is important to calibrate and dilate the urethra with sounds or bougies to accommodate the pediatric cystoscope and avoid trauma to the urethra. It is rarely necessary to perform a meatotomy to allow passage of the pediatric-size cystoscopes.

Fig. 26.3
Pediatric endoscopic table with pediatric-size stirrups
Ureterocele
During cystourethroscopy, it is important to view the urethral anatomy and bladder anatomy with the bladder empty and full. This avoids effacement or compression of the ureterocele when the bladder is distended. Maneuvers to distend the ureterocele may be helpful such as manually compressing the ipsilateral flank. As demonstrated in the accompanying video, we make a small incision or puncture near the base of the ureterocele. This incision site theoretically allows the superior tissue to serve as a “flap-valve” mechanism preventing iatrogenic vesicoureteral reflux. Adequate decompression of the ureterocele is the goal of endoscopic treatment of ureteroceles, but an overaggressive incision or puncture will result in an increased chance vesicoureteral reflux (Video 26.1).
Syringocele
We find the classification that differentiates syringoceles as either open or closed useful in the planning for endoscopic treatment [11] (Fig. 26.4). The closed-type syringocele may be incised for decompression using the same probes utilized for treatment of ureteroceles as described above. Open-type syringoceles may be unroofed by either employing a right-angle probe with cystoscopy or using an infant resectoscope.
Fig. 26.4
Simple classification of types of syringoceles (Cowper’s duct cysts). (a) Closed type. (b) Open type
Postoperative Management
We do not typically employ any drainage after endoscopic treatment of ureteroceles. Children are placed on antibiotic prophylaxis and are followed up in the clinic with ultrasonography to document decompression. A micturition cystourethrogram is obtained to rule out iatrogenic vesicoureteral reflux. When evidence of decompression is verified and vesicoureteral reflux is excluded, antibiotic prophylaxis is stopped. Further follow-up is performed with ultrasonography and clinical assessment accordingly.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


