The management of endometrial cancer has changed significantly over the last 40 to 50 years. During the 1970s, endometrial cancer was clinically staged. Patients with early-stage disease were treated with preoperative packing of the endometrial cavity with radiation sources, Heyman capsules, followed by hysterectomy. In 1988, the International Federation of Gynecology and Obstetrics (FIGO) approved a surgical staging system for endometrial cancer. This acknowledged the shift to surgery as primary therapy, with pelvic radiotherapy being used postoperatively as adjuvant therapy for women at increased risk for recurrence. The FIGO staging system for endometrial cancer was again revised in 2009 to reflect our improved understanding of the prognostic factors for this disease. The role of lymphadenectomy and postoperative radiotherapy in the treatment of patients with endometrial cancer remains controversial. Laparoscopic surgery, particularly robotic-assisted laparoscopy, is becoming more important in the treatment of this disease.
In 1983, JV Bokhman described two pathogenetic types of endometrial cancer. Type I tumors account for approximately 90% of endometrial cancers and are associated with exposure to unopposed estrogen from either internal or external sources. They are typically of endometrioid pathology, low grade, diagnosed at early stage, and have an excellent prognosis. Type II tumors are high grade and often have papillary serous or clear cell pathology. They tend to be diagnosed at a later stage, but have a poor prognosis even if diagnosed at an early stage. There is a clear difference in the molecular biology of these tumors. Type I tumors may be associated with a number of genetic changes, including microsatellite instability (20% to 45%), inactivation of the PTEN tumor suppressor gene (57% to 83%), PIK3CA mutation (up to 50%), PIK3R1 mutation (20% to 40%), EGFR overexpression (38% to 46%), E-cadherin loss (6% to 57%), mutational activation of the K-ras oncogene (22% to 43%), BAF250a loss (29% to 39%), and gain of function mutation of the β-catenin gene (14% to 47%). Type II tumors are characterized by aneuploidy. Overall, 9% to 54% of type II tumors exhibit inactivating mutations of p53 gene locus. However, in serous endometrial cancers, over 90% demonstrate p53 inactivation. Type II endometrial cancers may show other mutations, such as PIK3CA (30%), PIK3CA amplification (45%), HER2 amplification (17% to 50%), EGFR overexpression (35% to 56%), E-cadherin loss (41% to 87%), and BAF250 loss (18% to 26%).
EPIDEMIOLOGY
According to American Cancer Society (ACS) estimates, endometrial cancer remains the most common of the gynecologic malignancies in the United States, with 52,630 new cases anticipated in 2014. This makes it the fourth most common cancer occurring in women, behind only breast, lung, and colorectal cancer. It is estimated that there will be 8,590 deaths due to endometrial cancer in the year 2014. That most women with newly diagnosed endometrial cancer can expect a good prognosis is due to the fact that endometrial cancer is usually diagnosed at an early stage, when it is readily treatable with surgery alone. However, there remain a few patients with endometrial cancer who present with high-risk histologic subtypes or advanced stage disease, in whom the prognosis is more guarded. Table 52.1 shows the stage distribution and survival of patients diagnosed with endometrial cancer from 1999 to 2001, as reported in the 26th annual FIGO report.
TABLE 52.1 Stage and Survival of Endometrial Cancer
STAGE
PATIENTS
5-YR SURVIVAL
I
70%
89.6%
II
13%
78.3%
III
14%
61.9%
IV
3%
21.1%
The 2009 FIGO staging system for endometrial cancer as described by Pecorelli et al. is shown in Table 52.2. Tumor grade and depth of myometrial invasion are important prognostic features for endometrial cancer. In the 1988 surgical staging system, tumors confined to the uterine corpus had been divided into three groups: (a) those with no invasion, (b) those with less than 50% myometrial invasion, and (c) those with greater than 50% myometrial invasion. Because FIGO data demonstrated no significant difference in 5-year survival between patients with grade 1 or grade 2 tumor without myometrial invasion as compared to patients with grade 1 or grade 2 tumor with less than 50% myometrial invasion, these two groups were combined.
The 2009 FIGO staging system for endometrial cancer no longer upstages a patient for extension to the endocervical glands. Stage II tumors are now defined as those that invade the cervical stroma. Tumors involving the endocervical glands only are classified as stage I and subdivided according to the depth of myometrial invasion.
The 1988 FIGO staging system had defined patients with positive peritoneal washings as having stage IIIA disease. Positive peritoneal washings are associated with a worse prognosis only in patients with other adverse prognostic features. The presence of malignant cells in the peritoneal washings has been demonstrated not to be an independent adverse prognostic variable. Thus, it has been removed from the staging system. Peritoneal washings should still be performed and reported on every patient with endometrial cancer. Extension to the parametrium has been added to vaginal metastases in stage IIIB.
Stage IIIC previously encompassed metastases to the pelvic and/or paraaortic lymph nodes. Many studies suggest a worse prognosis with spread to the paraaortic lymph nodes. Thus, stage IIIC has been subdivided into IIIC1, pelvic lymph node involvement only, and stage IIIC2, paraaortic lymph node involvement with or without pelvic lymph node involvement.
TABLE 52.2 FIGO Staging of Carcinoma of the Corpus Uteri, 2009
Stage I
Tumor Confined to the Corpus Uteri
IA
No or less than half myometrial invasion
IB
Invasion equal to or more than half of the myometrium
Stage II
Tumor invades cervical stroma, but does not extend beyond the uterus
Stage III
Local and/or regional spread of tumor
IIIA
Tumor invades the serosa of the corpus uteri and/or adnexa
IIIB
Vaginal and/or parametrial involvement
IIIC
Metastases to pelvic and/or paraaortic lymph nodes
IIIC1
Positive pelvic lymph nodes
IIIC2
Positive paraaortic lymph nodes with or without positive pelvic lymph nodes
Distant metastases, including intraabdominal metastases and/or inguinal lymph nodes
Positive cytology has to be reported separately without changing the stage.
Histopathology: Degree of Differentiation
Grade 1
5% or less of a solid growth pattern
Grade 2
6%-50% of a solid growth pattern
Grade 3
More than 50% of a solid growth pattern
Notable nuclear atypia, inappropriate for the architectural grade, raises the grade of a grade 1 or grade 2 tumor by 1.
Uterine papillary serous carcinomas and clear cell carcinomas of the endometrium are always high-grade tumors, by definition.
Uterine sarcomas account for less than 10% of all uterine cancers. The more common histologic types of uterine sarcoma include leiomyosarcoma, endometrial stromal sarcoma, high-grade undifferentiated sarcoma, and adenosarcoma. Prior to the revision of the FIGO staging system in 2009, uterine sarcomas had been staged using the same staging system as endometrial cancers. However, uterine sarcomas and endometrial cancers have significantly different patterns of spread and prognostic features. In the revised 2009 staging system, FIGO introduced a separate staging system for uterine sarcomas (Table 52.3). Carcinosarcoma, also known as malignant mixed müllerian tumor, was previously classified as a sarcoma but is now understood to be a poorly differentiated endometrial carcinoma. Therefore, malignant mixed müllerian tumors are staged according to endometrial cancer staging system.
Tumor extends beyond the uterus, within the pelvis
IIA Adnexal involvement
IIB Involvement of other pelvic tissues
III
Tumor invades abdominal tissues (not just protruding into the abdomen)
IIIA 1 site
IIIB >1 site
IIIC Metastases to pelvic and/or paraaortic lymph nodes
IV
Tumor with
IVA Bladder and/or rectum invasion
IVB Distant metastases
Adenosarcomas
Stage definition
I
Tumor limited to uterus
IA Tumor limited to endometrium/endocervix with no myometrial invasion
IB ≤ half myometrial invasion
IC > half myometrial invasion
II
Tumor extends beyond the uterus, within the pelvis.
IIA Adnexal involvement
IIB Involvement of other pelvic tissues
III
Tumor invades abdominal tissues (not just protruding into the abdomen).
IIIA 1 site
IIIB >1 site
IIIC Metastases to pelvic and/or paraaortic lymph nodes
IV
Tumor with
IVA Bladder and/or rectum invasion
IVB Distant metastases
Carcinosarcomas
Carcinosarcomas should be staged as carcinomas of the endometrium.
a Note: Simultaneous endometrial stromal sarcomas of the uterine corpus and ovary/pelvis in association with ovarian/pelvic endometriosis should be classified as independent primary tumors.
RISK FACTORS
There are no clear risk factors for type II endometrial cancers. Type I endometrial cancers are usually related to exposure to unopposed estrogen, whether exogenous or endogenous. Risk factors for type I tumors are summarized in Table 52.4. Endometrial cancer incidence increases with age, until about 70 years, when rates begin to decline. Living in North America or Northern Europe is associated with an increased risk of endometrial cancer.
Reproductive factors are associated with an increased risk of endometrial cancer. Endometrial cancer risk is increased in women who are nulliparous or infertile or have menstrual irregularities. Early onset of menarche or late age at menopause is also associated with an increased risk of endometrial cancer.
Exogenous exposure, such as estrogen replacement therapy, has been shown to be associated with an increased risk of endometrial cancer in a number of studies. A meta-analysis that combined data from both case-control and cohort studies found a 2.3-fold increased risk of endometrial cancer among women who had ever used estrogen replacement therapy as compared to never users. The risk increases with increasing estrogen dose and increasing duration of estrogen use. In the same meta-analysis noted above, the relative risk of developing endometrial cancer rose to 9.5 among women who had used estrogen replacement therapy for 10 or more years as compared to never users. The risk can be reduced by the concurrent use of cyclic or continuous progestin.
TABLE 52.4 Risk Factors for the Development of Endometrial Cancer
Increased risk
Increasing age
Residence in North America or Northern Europe
Higher socioeconomic status
Higher level of education
White race
Nulliparity
Infertility
Menstrual irregularities
Early menarche
Late menopause
Treatment with unopposed estrogen
Tamoxifen use
Anovulatory disorders, such as polycystic ovarian syndrome
Estrogen-producing tumors, such as granulosa-theca cell tumors
Obesity
Hypertension
Diabetes
High fat diet
Hereditary nonpolyposis colon cancer syndrome
Decreased risk
Oral contraceptive use
Nonmedicated plastic or copper IUD use
Consumption of some phytoestrogens, such as isoflavones and lignans
Diet rich in fruits, vegetables, and fiber
Physical activity
Cigarette smoking
The use of tamoxifen by postmenopausal women for the prevention or treatment of breast cancer is associated with an approximately twofold increased risk of endometrial cancer as well as an increased risk of uterine sarcoma. However, this small increased risk of uterine cancer is outweighed by the survival benefit of tamoxifen use among women with breast cancer. As compared to other endometrial cancers, tamoxifen-related endometrial cancers are not associated with an increased incidence of adverse prognostic features. Although tamoxifen acts as a weak estrogen in the postmenopausal endometrium, it has predominantly antiestrogenic effects in the premenopausal endometrium. Thus, there is no increased risk of endometrial cancers among premenopausal women using tamoxifen. The use of aromatase inhibitors for the treatment of breast cancer has not been associated with an increased risk of endometrial cancer.
Patient metabolic factors such as obesity are associated with an increased risk of endometrial cancer and an increased risk of mortality from the disease. Weiderpass et al. found that as compared to women of normal body mass index (BMI), women with a BMI of 30 to 33.99 had a threefold increased risk of endometrial cancer that rose to a sixfold increased risk among women with a BMI greater than 34. In the Million Women Study, the relative risk of developing endometrial cancer was 2.73 and the relative risk of dying of endometrial cancer was 2.28 among women with a BMI ≥ 30 as compared to women with a normal BMI. Likewise, in a large prospective study of the effect of obesity on the risk of death from cancer, Calle et al. found that the relative risk of death from endometrial cancer was increased over sixfold among women with a BMI ≥ 40 as compared to those with a normal.
In the past, the increased risk of endometrial cancer among obese women has been attributed to increased levels of unopposed estrogen due to peripheral conversion of androgen to estrogen by the aromatase enzyme in adipose tissue. More recently, the roles of proinflammatory adipokines, which are cytokines produced in the adipose tissues, and of insulin and insulin-like growth factor on stimulating endometrial cancer development have begun to be elucidated.
The ovaries may be a source of unopposed estrogen in women with anovulatory disorders, such as polycystic ovarian syndrome (PCOS). In a retrospective study of 128 women with endometrial cancer, Pillay and colleagues found that among women less than 50 years old, PCOS was significantly more prevalent among women with endometrial cancer than among normal controls. They observed no relationship between PCOS and endometrial cancer in postmenopausal women.
Fearnley et al. conducted a case-control study of the incidence of endometrial cancer in 156 women with PCOS as compared to 398 controls. They identified a statistically significant fourfold increased risk of endometrial cancer among women with PCOS. After controlling for BMI, the difference in endometrial cancer risk did not remain significant. Therefore, some experts contend that PCOS, per se, is not a risk factor for endometrial cancer. They emphasize that women with PCOS have multiple other risk factors for endometrial cancer, including chronic anovulation, centripetal obesity, and diabetes. Premenopausal women with PCOS should be counseled on the risk of endometrial cancer and the importance of maintaining regular withdrawal bleeding cycles. The optimal treatment regimen is unknown (ACOG Practice Bulletin 108). Estrogen-producing tumors, such as granulosa cell tumors of the ovary, may be another source of endogenous, unopposed estrogen, and endometrial hyperplasia or cancer is common in women with estrogen-producing tumors.
The risk of endometrial cancer is increased in patients with diabetes. This risk is further increased in obese diabetic patients. Similarly, the risk of endometrial cancer is increased in patients with metabolic syndrome. Of the components of the metabolic syndrome, elevated BMI is the factor most strongly associated with endometrial cancer risk.
Factors that decrease exposure to unopposed estrogens decrease the risk of endometrial cancer. The Cancer and Steroid Hormone Study demonstrated that 12 months of oral contraceptive use decreased the risk of endometrial cancer by 40%, and the effect persisted for at least 15 years after the cessation of use. A large, Chinese case-control study demonstrated a 50% decrease in the risk of endometrial cancer after 3 years of oral contraceptive use.
Smoking also decreases the risk of endometrial cancer. The exact mechanism is unknown. It may be due to alterations in sex hormone metabolism, a reduction in body weight among smokers, or an earlier age at menopause among smokers. Obviously, the overall detrimental health effects of smoking far outweigh any benefit related to decreased endometrial cancer risk.
A number of studies have suggested a protective effect of IUD use on the risk of endometrial cancer. Tao’s large case-control study of 2,416 women in Shanghai, China, demonstrated an approximately 50% reduction in the risk of endometrial cancer among women who had ever used an intrauterine device (IUD). The type of IUD was not specified. Case-control studies by Castellsague in patients using unspecified type of IUDs and by Hill in patients using nonhormonal IUDs demonstrated a similar approximately 50% decreased risk of endometrial cancer in IUD users as compared to nonusers.
Gardner et al. conducted a randomized controlled trial of levonorgestrel IUD versus observation in 122 postmenopausal women with breast cancer who were being treated with tamoxifen. The mean follow-up time was 26 months, range 14 to 36 months. They were able to demonstrate benign endometrial changes and a decrease in the development of endometrial polyps in the IUD users as compared to nonusers. This study was unable to assess the effect of IUD use on the development of endometrial cancer. Nor could this study assess the safety of levonorgestrel-containing IUD use in women with breast cancer.
Endometrial cancer is one of the components of the Lynch syndrome. This autosomal, dominant cancer risk syndrome is caused by inactivation of one of several genes involved in DNA mismatch repair. A personal and/or family history of colon, endometrial, ovarian, ureteral, or smallbowel malignancy should prompt the clinician to consider referral of the patient for genetic counseling and possible genetic testing. Diagnosis of an endometrial or ovarian cancer often triggers the identification of a family with Lynch syndrome.
The lifetime risk of endometrial cancer in women with Lynch syndrome is 40% to 60%. Patients with Lynch syndrome may consider chemoprevention with OCPs, although there are no clear data to support this approach. A woman with Lynch syndrome may consider increased surveillance with annual endometrial biopsy beginning at age 30 to 35, although there is no definitive evidence to support this approach. Patients should be counseled to promptly report and be evaluated for any abnormal uterine bleeding. Risk-reducing surgery with hysterectomy and bilateral salpingo-oophorectomy (BSO), performed after the completion of childbearing, has been demonstrated to reduce the risk of endometrial cancer in patients with Lynch syndrome.
PROGNOSTIC FEATURES
The prognostic features for endometrial cancer have been well defined (Table 52.5). These include age, race, FIGO stage, tumor grade, histologic subtype, depth of myometrial invasion, cervical or adnexal involvement, positive peritoneal cytology, metastasis to pelvic or paraaortic lymph nodes, and presence of lymphovascular space invasion.
Among women with stage I endometrial cancer, risk factors that adversely affect survival include increasing age, grade 2 to 3 histology, the presence of lymphovascular space invasion, and invasion to the outer third of the myometrium. Using these factors, patients with “high-intermediate risk” for recurrence can be identified. These patients have an approximately 27% chance of recurrence at 48 months. The GOG defines high-intermediate risk endometrial cancer as (a) any age with greater than or equal to 3 or more risk factors; (b) age greater than or equal to 50 but less than 70 with greater than or equal to 2 or more risk factors, and (c) age greater than or equal to 70 with greater than or equal to 1 or more risk factors (Keys). Many experts suggest that these are the patients who should be targeted for surgical staging and/or postoperative adjuvant therapy.
TABLE 52.5 Prognostic Features for Endometrial Cancer
Metastases to the pelvic or paraaortic lymph nodes
Lymphovascular space invasion
DNA aneuploidy
a Denotes prognostic features that are most important in patients with endometrial cancers confined to the uterus.
SCREENING FOR ENDOMETRIAL CANCER
The ACS guidelines for the early detection of cancer recommend that for average-risk, asymptomatic individuals, endometrial cancer screening should consist of education of women at the time of menopause regarding the risks and symptoms of endometrial cancer. Women should be strongly encouraged to report any unexpected bleeding or spotting to their physician.
Even women at increased risk for endometrial cancer due to a history of unopposed estrogen therapy, tamoxifen use, late menopause, nulliparity, infertility, anovulation, obesity, diabetes, or hypertension do not benefit from routine screening for endometrial cancer, beyond the reporting of symptoms. The ACS recommends that women at high risk for endometrial cancer, such as women known or at substantial risk to be a carrier of a Lynch syndrome mutation, should be offered annual screening with endometrial biopsy by the age of 35, in addition to being informed about the symptoms of endometrial cancer. Patients should be counseled regarding the potential benefits, risks, and limitations of endometrial cancer screening. These recommendations are based on expert opinion. There is no current evidence that this approach will result in earlier diagnosis or improved outcomes for these women.
EVALUATION OF THE SYMPTOMATIC PATIENT
Abnormal uterine bleeding is the most common presenting symptom of endometrial cancer. In a review of the pathologic findings among women with postmenopausal bleeding, Gredmark and colleagues found that the risk of adenomatous endometrial hyperplasia or cancer in a woman with postmenopausal bleeding is approximately 18%. The risk of malignancy increased with increasing age, with the peak incidence of endometrial cancer occurring in women between 65 and 69 years of age. The most common cause of postmenopausal bleeding was endometrial atrophy, which was identified in 50% of the patients. All patients with postmenopausal bleeding should undergo evaluation for possible endometrial cancer.
Endometrial cancer can also occur in premenopausal women and may present with heavy or irregular vaginal bleeding. The American Congress of Obstetricians and Gynecologists recommends that any women aged 45 or older with abnormal bleeding should have endometrial sampling performed. Younger women with risk factors for endometrial cancer, such as obesity or anovulation, who have failed hormonal treatment, or who have persistent abnormal uterine bleeding should also undergo endometrial sampling. A 25-year-old woman who experienced menarche at age 12, is obese, and has PCOS will already have experienced more than 10 years of exposure to unopposed estrogen.
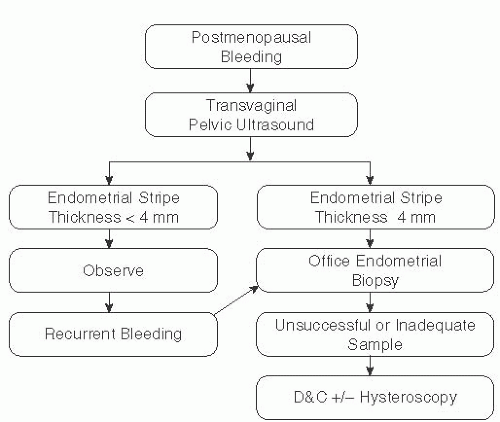
There are several options for the evaluation of a woman with postmenopausal bleeding. The ACOG Committee Opinion on the assessment of postmenopausal bleeding recommends either transvaginal pelvic ultrasonography or office endometrial biopsy as the initial approach, but not both together (Fig. 52.1).
Transvaginal pelvic ultrasound to evaluate the endometrial stripe thickness is one of the options for primary evaluation of postmenopausal bleeding. Several meta-analyses have been published evaluating the use of transvaginal pelvic ultrasound in the triage of women with postmenopausal bleeding. The most referenced meta-analysis, performed by Smith-Bindman et al., evaluated 35 studies performed between 1966 and 1996 that included 5,892 patients. Women with a pretest probability of cancer of 10% had only a 1% risk of having cancer following a transvaginal ultrasound result showing 5 mm or less endometrial stripe.
Gupta et al. performed a subsequent meta-analysis that assessed 57 studies in 9,031 postmenopausal women. Only four studies using a cutoff of less than or equal to 5 mm were of adequate quality to be included in the analysis. They found that among women with an endometrial stripe thickness of 5 mm or less, the risk of endometrial cancer was approximately 2.5%.
Timmermans et al. performed a meta-analysis using original datasets from 13 studies including 2,896 patients. They calculated receiver operating characteristic curves of endometrial thickness. The commonly used cutoff values of 4 and 5 mm were found to have a sensitivity to detect endometrial cancer of 95% and 90%, respectively. These authors recommend the use of a 3-mm cutoff value, which yielded a sensitivity of 98% for the detection of endometrial cancer.
ACOG recommends that endometrial sampling is not required in a patient with postmenopausal bleeding and an endometrial stripe thickness of less than or equal to 4 mm. If the endometrial stripe thickness is greater than 4 mm or if the endometrial stripe thickness cannot be assessed, then further evaluation with endometrial biopsy, sonohysterography to rule out endometrial polyps or submucosal fibroids, or office hysteroscopy is indicated.
Another option for the initial evaluation of postmenopausal vaginal bleeding is to proceed directly to office endometrial biopsy. This is typically accomplished with a Pipelle instrument, which is a disposable plastic catheter that can be placed through the cervix into the endometrial cavity for the aspiration of endometrial cells. Its use occasionally may require the placement of a single-toothed tenaculum on the cervix for countertraction or gentle cervical dilatation.
In a meta-analysis comparing endometrial sampling techniques, the Pipelle was found to be the most accurate. Among postmenopausal women, the sensitivity for the detection of atypical endometrial hyperplasia was 81% and for the detection of endometrial cancer was 99.6%. The sensitivity of the device for the detection of endometrial cancer among premenopausal women was 91%. The specificity of the Pipelle device for the diagnosis of endometrial hyperplasia or malignancy was 98%.
Up to 54% of patients will have failure of endometrial sampling. Farrell and coworkers have reported a 20% incidence of uterine pathology after an “insufficient” endometrial biopsy, with 3% of these patients having malignancy. These patients may be further evaluated with transvaginal pelvic ultrasound. If the stripe thickness is ≤4 mm, then the risk of malignancy is low (Farrell).
Dilatation and curettage (D&C) in the operating room is considered the “gold standard” for endometrial sampling. However, even D&C fails to sample the entire endometrial cavity. Stock and Kanbour performed prehysterectomy D&Cs and found that in approximately 60% of patients, less than half of the endometrium had been sampled. There are limited data regarding the sensitivity and specificity of D&C for the diagnosis of endometrial hyperplasia and malignancy. Women with persistent postmenopausal bleeding despite a negative prior workup should undergo reevaluation.
Both Pipelle endometrial biopsy and D&C are limited for the evaluation of focal endometrial lesions. Studies differ as to whether adding hysteroscopy may improve the diagnostic accuracy of D&C. Patients with endometrial cancer who undergo hysteroscopy are more likely to have positive pelvic peritoneal washings than those who do not undergo hysteroscopy, which may be due to insufflation of the uterus with fluid during hysteroscopy. There is currently no evidence that this results in an increased risk of recurrence or decreased survival. This conclusion is limited by the small number of patients with recurrent disease and short follow-up intervals.
ENDOMETRIAL HYPERPLASIA
Endometrial hyperplasia is a proliferation or overgrowth of the endometrium caused by exposure to unopposed estrogen. Kurman et al. further classified endometrial hyperplasia into four groups, simple hyperplasia with and without atypia and complex hyperplasia with or without atypia. Simple hyperplasia is characterized by an increase in the number of endometrial glands, which may be dilated with little crowding or may have irregular outline and exhibit crowding. Complex hyperplasia is characterized by glands with irregular outline that demonstrate marked structural complexity and back-to-back crowding. Atypical hyperplasias demonstrate cytologic atypia and loss of cellular polarity. These criteria were adopted by the World Health Organization for the classification of endometrial hyperplasia in 1994.
More recently, Muter and colleagues have introduced a two-tier system for the classification of premalignant lesions of the endometrium, the endometrial intraepithelial neoplasia system. This system uses morphometric analysis to differentiate between monoclonal, premalignant lesions as compared to polyclonal and not premalignant lesions. In this system, the lesion must exceed 1 mm, the area of glands exceeds that of the stroma, and the cytology differs between the architecturally crowded focus and the background endometrial glands. Cytologic atypia is associated with an increased risk of progression to endometrial cancer. In Kurmans’s series of 170 women with endometrial hyperplasia not treated with progesterone, progression to cancer occurred in 1% of patients with simple hyperplasia without atypia, 3% of patients with complex hyperplasia without atypia, 8% of patients with simple hyperplasia with atypia, and 29% of patients with complex hyperplasia with atypia during a mean follow-up time of 13.4 years. In another study by Horn et al., among women with complex hyperplasia without atypia, only 2% progressed to cancer and 10.5% progressed to complex atypical endometrial hyperplasia. Among women with complex hyperplasia without atypia treated with progestin therapy, 128 of 208 (61.5%) regressed. Progression to cancer occurred in 58 of 112 women (52%) with complex atypical hyperplasia. Of the seven patients with complex atypical endometrial hyperplasia treated with progestins, four had persistent disease and three progressed to cancer.
Endometrial hyperplasias without atypia are typically treated with some form of progestin therapy. Common regimens include medroxyprogesterone acetate 10 to 20 mg daily or cyclically for 14 days per month, depot medroxyprogesterone 150 mg intramuscularly every 3 months, megestrol acetate 40 to 160 mg daily, or the levonorgestrel-containing IUD (Trimble).
Complex atypical hyperplasia of the endometrium is a premalignant condition, which is typically treated with hysterectomy with or without BSO. Approximately 40% of women with complex atypical endometrial hyperplasia diagnosed by biopsy will have the finding of endometrial cancer in the hysterectomy specimen. The risk of change in diagnosis from hyperplasia to cancer may be slightly higher with preoperative Pipelle endometrial biopsy (46%) than with D&C (27%).
Progestin therapy can be considered for women with complex atypical endometrial hyperplasia or in selected women with grade 1 endometrial cancer who are either poor operative candidates or who wish to retain their fertility. Gunderson and colleagues performed a systematic review of 45 published studies including a total of 391 women, 111 with complex atypical endometrial hyperplasia and 280 with grade 1 endometrioid adenocarcinoma of the endometrium who were treated with progestin therapy. The median age of the patients was 31.7 years in trials for which patient age was reported. Median follow-up was 39 months. The most common progestins used were medroxyprogesterone in 49%, megestrol acetate in 25%, and levonorgestrel-containing IUD in 19%. The complete response rate was 65.8% in women with complex atypical endometrial hyperplasia and 48.2% in women with endometrial cancer. The median time to complete response was 6 months. Recurrence was diagnosed in 23.2% of women with hyperplasia and 35.4% of women with cancer. There were 117 live births among the 391 women in this study.
Before progestin therapy is considered in a young woman with complex atypical endometrial hyperplasia or grade 1 endometrial cancer who is attempting to retain her fertility, a thorough evaluation of the endometrial cancer by D&C should be performed. If endometrial cancer is confirmed, then transvaginal pelvic ultrasound and magnetic resonance imaging (MRI) of the pelvis should be performed to rule out myometrial invasion and any ovarian pathology. Chest x-ray or chest computed tomography (CT) with CT of the abdomen and pelvis should be performed to evaluate for the possibility of metastatic disease. Patients with hyperplasia or cancer who are being treated with progestins should have endometrial sampling every 3 months to evaluate response to therapy. They should be extensively counseled regarding the risks of this approach. There is a case report describing progression to grade 2 endometrioid adenocarcinoma of the endometrium metastatic to the lymph nodes in a 40-year-old patient with complex atypical hyperplasia who was treated with progestin.
SURGICAL STAGING AND TREATMENT
Rationale
Endometrial cancer is surgically staged and treated. The procedure includes thorough exploration of the peritoneal contents, pelvic washings, hysterectomy, and BSO. The role of bilateral pelvic and paraaortic lymph node dissection remains controversial. Laparotomy has been the principle surgical approach to hysterectomy and staging for endometrial cancer. Laparoscopy and robotically assisted laparoscopy are increasingly being used for endometrial cancer surgery. Since laparoscopic hysterectomy and lymph node dissection techniques are discussed in detail elsewhere in this text, the discussion below will focus on open techniques.
Type I endometrial cancers have three main patterns of spread, by direct extension, to regional lymph nodes, and hematogenously. The most common mechanism of spread for type I endometrial cancer is by direct extension, invading into the myometrium or by extension to the adjacent cervix. Hematogenous metastasis tends to occur late in the course of the disease. Type II endometrial cancers, particularly uterine papillary serous carcinomas, may also metastasize within the peritoneal cavity, similar to ovarian carcinomas.
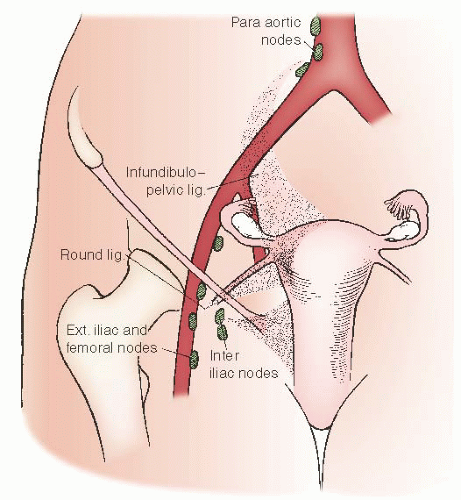
Endometrial carcinoma spreads through three separate lymphatic pathways: Paracervical and parametrial lymphatics drain to the pelvic lymph nodes, ovarian lymphatics drain to the paraaortic lymph nodes, and round ligament lymphatics drain to the inguinal lymph nodes (Fig. 52.2). The lymphatic drainage of the uterine fundus and cervix directs most of the metastases to the pelvic lymph nodes. Although the paraaortic lymph nodes may be primary metastatic sites via spread through the infundibulopelvic ligament lymphatics, it is rare for an endometrial cancer patient to have isolated paraaortic lymph node metastases without concomitant pelvic lymph node metastases. The incidence of isolated paraaortic lymph node metastases is approximately 1% to 1.5%.
Performance of pelvic and paraaortic lymphadenectomy for the staging of endometrial cancer remains controversial. Kilgore and colleagues retrospective study suggested that lymphadenectomy might have a therapeutic effect for patients with endometrial cancer. They evaluated the outcomes of 649 patients surgically managed for endometrial cancer. In this study, 212 patients had pelvic lymph nodes sampled from at least 4 separate sites (multiple-site lymph node sampling), 205 patients had pelvic lymph nodes sampled from fewer than 4 sites (limited-site lymph node sampling), and 208 patients had no pelvic lymph nodes sampled. Patients undergoing multiple-site lymph node sampling had a survival of approximately 85%, whereas patients in whom pelvic lymph nodes were not sampled had a survival of approximately 65%, a statistically significant difference (P = 0.0027). This survival advantage for patients with multiple-site lymph node sampling persisted even in a subgroup analysis of patients treated with postoperative whole pelvic radiotherapy.
FIGURE 52.2 Lymphatic pathways of tumor spread of endometrial carcinoma to pelvic and extrapelvic nodes.
There have been two prospective randomized trials assessing the therapeutic value of pelvic lymphadenectomy in patients with apparent stage I endometrial cancer. The ASTEC trial enrolled 1,408 patients at 85 centers in 4 countries. Median follow-up was 37 months. Patients were randomized to “standard surgery” with hysterectomy, BSO, washings, and palpation of the paraaortic lymph nodes versus standard surgery with pelvic lymphadenectomy. Postoperatively, patients were enrolled in a second randomized trial of postoperative radiotherapy versus no radiotherapy based on uterine findings. The overall morbidity was low, but patients in the lymphadenectomy group were more likely to develop lower extremity lymphedema. The authors reported that there was no difference in overall or recurrence-free survival in patients who did not undergo pelvic lymphadenectomy versus those who did.
This trial has been extensively criticized. Although the patients were randomized, there was an excess of patients with adverse prognostic features in the lymphadenectomy arm, including 10% more patients in the lymphadenectomy arm having deep myometrial invasion. The lymph node sampling itself was inadequate, with a median of only nine nodes being recovered. The Gynecologic Oncology Group Surgical Procedures Manual, revised January 2010, requires a minimum of four nodes from each side for an adequate pelvic lymph node dissection. The performance of paraaortic lymph node dissection was left to the discretion of the surgeon. Since the randomization to postoperative external beam radiotherapy was based on uterine factors and not the presence of metastases to the pelvic lymph nodes, approximately half of those who might have benefited the most from pelvic radiotherapy, those with lymph node metastases, did not receive it.
CONSORT was a phase III randomized trial of routine lymphadenectomy versus no lymphadenectomy in women with apparent stage I endometrial cancer who were undergoing standard surgery with hysterectomy and BSO. Paraaortic lymph node sampling was left to the discretion of the surgeon. Postoperative therapy was at the discretion of the treating physician, but was similar between the two groups. In this trial, the pelvic lymph node dissection was adequate by GOG standards with a median of 30 lymph nodes removed in the lymphadenectomy group. Intraoperative complications were similar. Patients in the lymphadenectomy group were more likely to experience postoperative complications, which was largely due to an excess of lymphedema and lymphoceles in the lymphadenectomy group. These authors also found no difference in overall or disease-free survival in the lymphadenectomy group. However, they did conclude that systematic lymphadenectomy significantly improved the accuracy of surgical staging.
In assessing the preceding studies, it is important to understand the purpose of staging. According to the SEER Web site, among the purposes of cancer staging is to “adequately assess the extent of cancer in order to treat the disease in the most appropriate manner.” The findings of a staging evaluation are used to direct therapy in order to maximize the chance of cure while minimizing the risk of toxicity. Using this paradigm, it may be appropriate to omit lymphadenectomy in patients with grade 1 endometrial cancer confined to the endometrium who have essentially no risk of lymph node metastases. In patients with high-intermediate risk disease, surgical staging may be useful to identify those patients with lymph node metastases who may benefit from radiotherapy, while avoiding short- and long-term radiotherapy toxicity in women who can be confirmed to have negative lymph nodes.
Ben-Shachar and coworkers evaluated the impact of routine surgical staging on the treatment of 181 women with a preoperative diagnosis of grade 1 endometrioid adenocarcinoma of the endometrium. Surgical staging was performed in 82% of cases and was omitted only when the disease was apparently confined to the endometrium and the surgical risk was high. High-risk uterine features, including greater than one-half myometrial invasion, grade 3 tumors, high-risk histologic variants, and/or cervical extension were identified in 26% of patients. Lymph node metastases were identified in 3.9% of patients. Overall, the findings of the surgical staging procedure significantly impacted postoperative treatment decisions in 29% of patients, including 12% of patients who were determined to need adjuvant therapy and 17% of patients who were able to forego external beam whole pelvic radiotherapy or chemotherapy. The incidence of severe surgical complications in the surgically staged group was 3.2%.
Preoperative Assessment and Preparation
As noted above, many patients with endometrial cancer may be older and have multiple medical comorbidities. Thus, preoperative preparation is important. All patients should have a thorough history and physical examination. The history should assess the length and severity of the patient’s bleeding or other presenting complaint. It should also assess for symptoms of metastatic disease, such as abdominal or pelvic pain, changes in bowel or bladder function, lower extremity pain or swelling, abdominal bloating, early satiety, shortness of breath, or cough. Previous medical history and symptoms suggestive of occult cardiopulmonary disease or other medical illnesses should be ascertained. Careful attention should be paid to the family history, as endometrial cancer may develop before colon cancer in up to half of women with Lynch syndrome.
Only gold members can continue reading. Log In or Register to continue