Ear, Painful
Christine S. Cho
INTRODUCTION
Diseases that produce ear pain are common maladies of childhood. Many cases of otalgia are caused by acute otitis media. Otitis externa is also commonly seen, especially during the summer months.
External Ear Pain
Infection
Otitis externa (swimmer’s ear)
Auricular cellulitis
External canal abscess
Infected preauricular sinus
Herpes simplex virus infection
Herpes zoster
Neoplasm
Neoplasms of the external auditory canal
Trauma
Lacerations
Hematoma or seroma
Frostbite and burns
Miscellany
Foreign body and cerumen impaction
Middle and Inner Ear Pain
Infection
Acute otitis media
Myringitis
Mastoiditis
Neoplasm
Rhabdomyosarcoma and lymphoma
Histiocytosis X
Trauma
Traumatic perforation
Barotrauma
Inflammation
Otitis media with effusion
Miscellany
Eustachian tube dysfunction
Cholesteatoma
Referred Pain
Infection
Dental abscess
Pharyngitis or tonsillitis
Stomatitis
Sinusitis
Cervical lymphadenitis
Retropharyngeal abscess
Peritonsillar abscess
Infected branchial cyst
Parotitis
Meningitis
Neoplasm
Neoplasms of the jaw, oropharynx, nasopharynx, larynx, facial nerve, or central nervous system
Trauma
Oral cavity, pharyngeal, laryngeal, or esophageal trauma or foreign body
Miscellany
Erupting teeth
Impacted teeth
Migraine
Temporomandibular joint dysfunction or arthritis
Bell palsy
DIFFERENTIAL DIAGNOSIS DISCUSSION
Acute Otitis Media
Etiology
Acute otitis media is an infection of the middle ear space that occurs when the eustachian tube obstructs and a build-up of fluid in the middle ear (effusion) gets infected by nasopharyngeal secretions. Obstruction can result from infection, allergy, enlarged adenoids, decreased eustachian tube stiffness, or inefficient tube opening. The most common pathogens are (in order of frequency) Streptococcus pneumoniae, nontypeable Haemophilus influenzae, and Moraxella catarrhalis. With the advent of the heptavalent pneumococcal conjugated vaccine, the incidence of otitis media from S. pneumoniae is decreasing; however, the long-term impact of the vaccine has yet to be established. Table 30-1 lists risk factors associated with acute otitis media.
Clinical Features
Symptoms of acute otitis media may include otalgia, fever, irritability (from the pain), vomiting, diarrhea, hearing loss, anorexia, and otorrhea. It is common for the patient to have a preceding upper respiratory infection.
 HINT: Parents commonly state that they are concerned about an ear infection because their child is, “pulling on their ears.” While many children with otitis media will rub or pull at their ears, this is not a specific sign of the disease.
HINT: Parents commonly state that they are concerned about an ear infection because their child is, “pulling on their ears.” While many children with otitis media will rub or pull at their ears, this is not a specific sign of the disease.TABLE 30-1 Risk Factors for Acute Otitis Media | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
Evaluation
To facilitate examination of the tympanic membrane, the clinician should properly position the child in his/her parent’s arms, lap, or on the examining table as well as manipulate the ear (i.e., pull the pinna posteriorly and superiorly and push the tragus forward by applying traction to the skin in front of the ear). See Figure 30-1 for ear anatomy. If necessary, remove cerumen with a curette or by irrigation with water. (However, irrigation is contraindicated when a perforated tympanic membrane is suspected.)
In acute otitis media, the tympanic membrane is opaque or cloudy, bulging, red, and has decreased mobility.
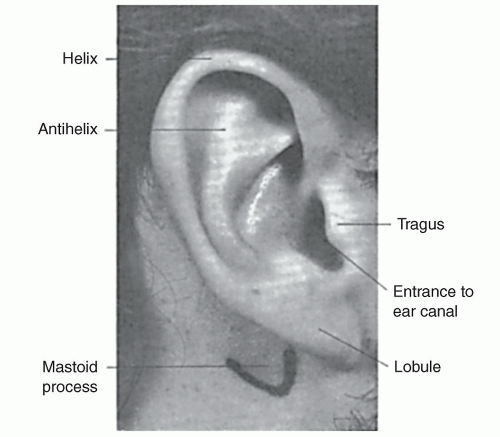 FIGURE 30-1 Anatomy of the ear. |
 HINT: Tympanic membrane erythema alone is not a reliable indicator of acute otitis media. A red tympanic membrane can also be caused by a viral upper respiratory tract infection, by crying, or by efforts to remove cerumen.
HINT: Tympanic membrane erythema alone is not a reliable indicator of acute otitis media. A red tympanic membrane can also be caused by a viral upper respiratory tract infection, by crying, or by efforts to remove cerumen.Tympanic membrane mobility should be assessed using tympanometry or pneumatic otoscopy—which involves applying positive and negative pressure to the tympanic membrane with a rubber bulb connected by a tube to the otoscope.
 HINT: To perform pneumatic otoscopy, use the largest speculum that will fit comfortably in the auditory meatus and fit the speculum tightly to the ear canal.
HINT: To perform pneumatic otoscopy, use the largest speculum that will fit comfortably in the auditory meatus and fit the speculum tightly to the ear canal.Laboratory evaluation is usually not necessary. Some clinicians do recommend that febrile infants with acute otitis media who are younger than 12 weeks undergo a full sepsis evaluation.
Treatment
Many patients who have physical findings consistent with the diagnosis of otitis media recover without treatment, and antibiotics afford only small improvement in symptom relief. Some experts recommend withholding antibiotic treatment for 48–72 hours and focusing on treatment of pain.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


