Fig. 52.1
Distribution of age in plicated and non-plicated patients (From Joho-Arreola et al. (2005) with permission)
In young infants under 6 months, plication should be performed after verification of the diagnosis. We developed an algorithm for these patients (Fig. 52.2) (Joho-Arreola et al. 2005). In our institution, we used a thoracic approach as described by Bisgard (Cilley and Coran 1995). In all patients with unilateral paralysis, plication was performed through the seventh intercostal space with a lateral thoracotomy and fixation of the diaphragm on the ventral tenth costal arch. In three cases with bilateral pareses, only one side was plicated similarly with good result. Our results are comparable with the findings of Lemmer et al. which showed in a study of 74 children with congenital heart disease and DP after operation that mechanical ventilation, ICU stay and hospital stay are prolonged in newborns and young infants without plication (Lemmer et al. 2007). Baker et al. performed in 17 patients after DP plication fluoroscopy assessing diaphragm motion. Excursion of the plicated diaphragm was 77 % of the contralateral side. There was a trend toward improved function over time (Baker et al. 2008).
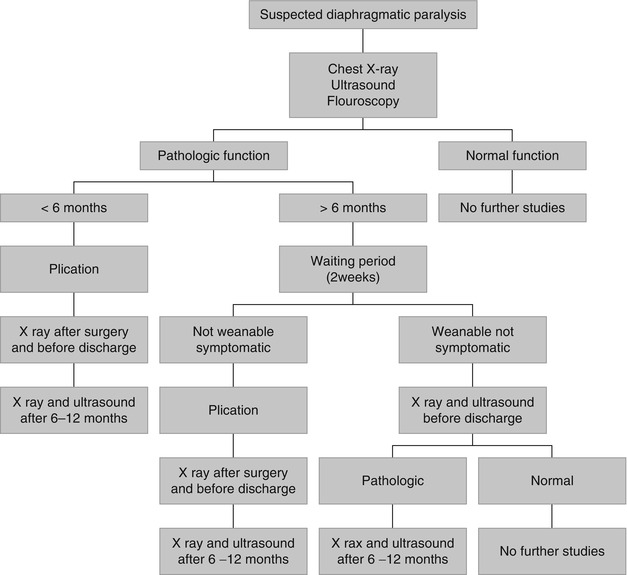
Fig. 52.2
Algorithm of patients with diaphragmatic paralysis (From Joho-Arreola et al. (2005) with permission)
In a follow-up of 22 adult patients, Versteegh et al. could show that the patients after plication improved in seated vital capacity, supine vital capacity and FEV1. On the transient dyspnoea index, a remarkable improvement was noted in dyspnoea (Versteegh et al. 2007).
In children undergoing univentricular heart repair with non-pulsatile circulation like after Fontan operation, early diaphragm fixation seems to reduce morbidity like pleural effusions, ascites, duration of hospital stay and need for readmission (Talwar et al. 2010). Video-assisted thoracoscopic plication of the diaphragm has been described in a small case series in children and adults with good results (Freeman et al. 2006; Hines 2003). Hines described five patients between one week and 2 years who were successfully operated with a short ICU stay time (Hines 2003).
Diaphragmatic pacing has been used in adults and older children but not in infants. It requires an intact phrenic nerve and is not an option in bilateral paralysis. It is usually used in children with a nonsurgical origin of paralysis.
Essential to Remember
Diaphragmatic paralysis is a typical complication after thoracic surgery and should be anticipated if babies cannot get off the ventilator.
In children older than 6 months, a conservative treatment is eligible.
Operative treatment is necessary in children under 6 months.
References
Affatato A, Villagra F, De Leon JP, Gomez R, Checa SL, Vellibre D, Sanchez P, Diez Balda JI, Brito JM (1988) Phrenic nerve paralysis following pediatric cardiac surgery. Role of diaphragmatic plication. J Cardiovasc Surg 29:606–609
Cilley RE, Coran AG (1995) Eventration of the diaphragm. In: Smith R (ed) Pediatric surgery. Chapman & Hall Medical, New York, pp 168–175
Gerscovich EO, Cronan M, McGahan JP, Jein K, Jones CD, McDonald C (2001) Ultrasonographic evaluation of diaphragmatic motion. J Ultrasound Med 20:597–604PubMed
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


