The intermediate mesoderm and the development of the urogenital organs in the early embryo (week 3)
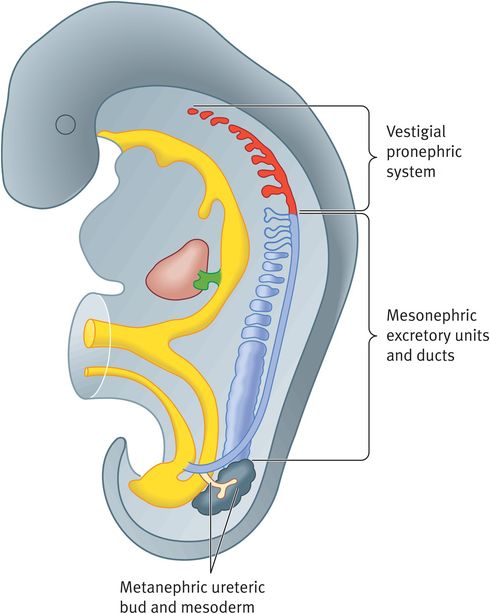
Schematic representation of the three types of excretory organs formed in the human embryo
The pronephros that appears at the beginning of week 4 of gestation is rudimentary and nonfunctional. It is seen as seven solid cell groups in the cervical region. All the elements of the pronephros disappear a week after their appearance. The pronephric ducts persist and are used by the mesonephros.
The mesonephros appears at week 4, becomes functional between weeks 6–10 and disappears by the end of week 10. The mesonephric ducts function as interim kidneys for 4 weeks (see Figure 12.4). They originate from the intermediate mesoderm between the upper thoracic and the upper lumbar segment (L3). They form excretory tubules that lengthen and acquire a tuft of capillaries. The tubules immediately adjacent to the vascular tuft differentiate into the Bowman’s capsule and, laterally, the tubules open into the wolffian duct. The tubules then degenerate but the wolffian ducts persist and participate in the formation of the genital system in the male but disappear in the female.
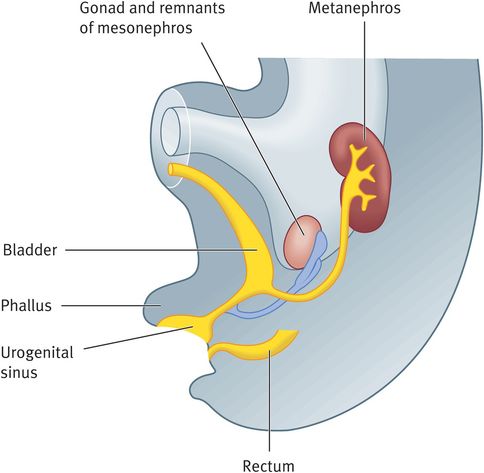
The metanephros forms the permanent kidney that appears in week 5 and urine production starts by week 12. The excretory units develop from the metanephric mesoderm (metanephric blastema). The collecting ducts develop from the ureteric bud, which is an outgrowth of the mesonephric duct close to its entrance to the cloaca. This bud penetrates the metanephric mesoderm, the stalk of the ureteric bud forms the ureter and the expanded part forms the renal calyx. Each newly formed collecting tubule is covered at its distal end by a metanephric tissue cap. The mesoderm adjacent to the collecting tubule develops into cells known as the metanephric vesicle. These vesicles differentiate later into the renal tubules and acquire a tuft of capillaries that later form glomeruli. Hence, the uriniferous tubule consists of the nephrons derived from the metanephric mass of intermediate mesoderm and a collecting tubule derived from the metanephric diverticulum. The glomerular integrity depends on signalling between the three major cell lineages: podocytes, and endothelial and mesangial cells. These tubules, together with their glomeruli, form nephrons. Hence, the kidney develops from two sources: metanephric mesoderm and the ureteric bud. In animal models, kidney formation is known to be controlled by the proteins RET (rearranged during transfection protooncogene), GDNF (giant cell line-derived neutrophilic factor) and GFRA1 (GDNF family receptor alpha-1) (Table 12.2). Mutations in RET are found in both unilateral (20%) and bilateral (37%) renal agenesis.
| Embryo | Adult derivatives |
|---|---|
| Pronephros | Not functional and completely regresses, paramesonephric duct forms internal genitalia of the female |
| Mesonephros | Completely regresses but the mesonephric duct forms the internal male genital organs |
| Metanephros | |
| Ureteric bud | Collecting duct, minor calyx, major calyx, renal pelvis, ureter (regulated by WT1, GDNF9 glial cell line-derived neurotrophic factor, C-RET9 tyrosine kinase receptor) |
| Metanephric mesoderm | Renal glomerulus, renal capsule, proximal convoluted tubule, loop of Henle, distal convoluted tubule, connecting tubule (regulated by fibroblast growth factor 2, bone morphogenetic protein 7, GFRA1, WNT11) |
Position of the Kidney
The kidney develops in the pelvic region and later ascends to a more cranial position. The change in position is due to the differential growth of the lumbar and sacral regions. As the kidney ascends, it rotates by 90 degrees and derives its blood supply from the aorta, and the lower vessels disappear.
Clinical correlates
Wilms tumour occurs as a result of mutation in WT1, which regulates the mesoderm to respond to induction by the ureteric bud.
Renal agenesis can occur if the ureteric bud fails to contact and/or induce the metanephric mesoderm. Unilateral renal agenesis occurs in 1 in 1000 infants. It is more common on the left side and in males. Unilateral renal agenesis is associated with a single umbilical artery. Bilateral renal agenesis is associated with oligohydramnios and characteristic facial appearance and occurs in 1 in 3000 births.
Duplication of the ureter results from early splitting of the ureteric bud. Splitting may be partial or complete and metanephric tissue may be divided into two parts, each with its own renal pelvis and ureter. Partial division results in a divided kidney with a bifid ureter and complete division results in a double kidney with a bifid ureter.
Accessory renal arteries occur from the persistence of embryonic vessels formed during the ascent of the kidney. About 25% of adult kidneys have two to four renal arteries. Accessory renal arteries usually arise from the aorta. Accessory arteries are about twice as common as accessory veins.
Polycystic kidney disease is an autosomal that occurs because of the wide dilatation of the nephrons, particularly the loop of Henle. Gene mutations and faulty signalling have been implicated.
Development of the bladder
During weeks 4 and 7 of development, the cloaca is divided into the urogenital sinus anteriorly and the anal canal posteriorly by the urogenital septum. The urogenital septum is a layer of mesoderm and its tip forms the perineal body. The urogenital sinus now develops into three parts. The cranial part forms the urinary bladder, which is continuous with the allantois. The narrower middle pelvic part forms the prostatic and membranous urethra in the male and the entire urethra in the female. The caudal, or phallic, part forms the genital organs (Figure 12.3). Later, the lumen of the allantois becomes obliterated to form the urachus (median umbilical ligament). During differentiation of the cloaca, caudal portions of the mesonephric ducts are absorbed into the wall of the urinary bladder. Consequently, the ureters outgrow the mesonephric ducts and enter the bladder separately. Since both mesonephric ducts and ureters originate in the mesoderm, the mucosa of the bladder (trigone) formed by the incorporation of the ureteric and ejaculatory ducts is mesodermal in origin.
The bladder after week 5
Development of the urethra
The epithelium of the urethra in both sexes originates in the endoderm; the surrounding connective and smooth muscle tissue is derived from the mesoderm. In males, the cranial part of the prostatic urethral epithelium forms numerous outgrowths that form the prostate. In females, the cranial part gives rise to the urethral and paraurethral glands.
Clinical correlates
When the lumen of the intraembryonic portion of the allantois persists, a urachal fistula drains urine into the umbilicus. If only a small area persists, then a urachal cyst is formed.
Congenital megacystis is a pathologically large bladder and results from maldevelopment of the ureteric bud. It is usually associated with renal failure and pulmonary hypoplasia unless intrauterine treatment is performed.
Exstrophy of the bladder is caused by a lack of mesodermal migration and incomplete closure of the inferior abdominal wall between the umbilicus and genital tubercle followed by rupture of the thin layer of ectoderm. It occurs in 10 in 40 000 births. The anomaly is characterised by protrusion of the posterior wall of the bladder. Complete exstrophy is associated with epispadias and wide separation of the pubic bones.
Exstrophy of the cloaca occurs because of the failure of migration of mesoderm to the midline. The defect includes exstrophy of the bladder, spinal defects, imperforate anus and usually omphalocele.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


