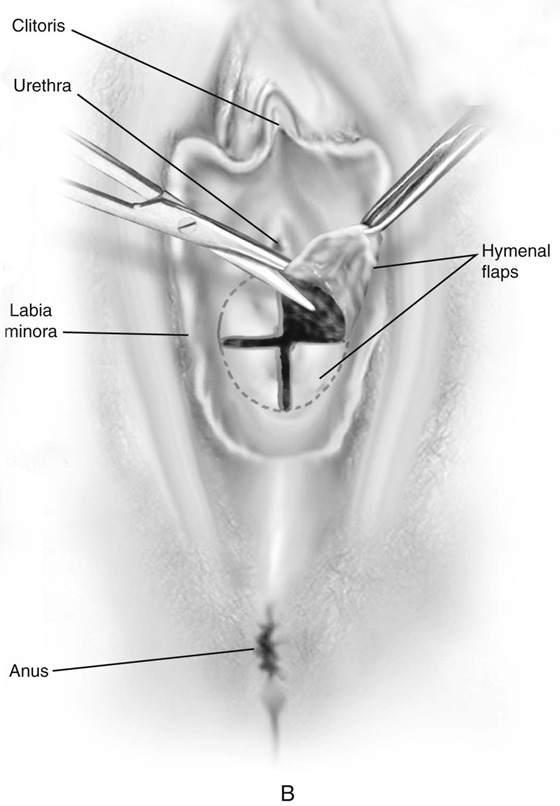
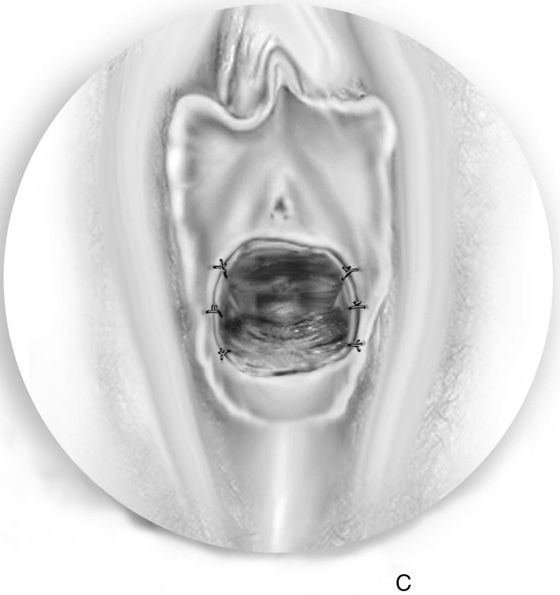
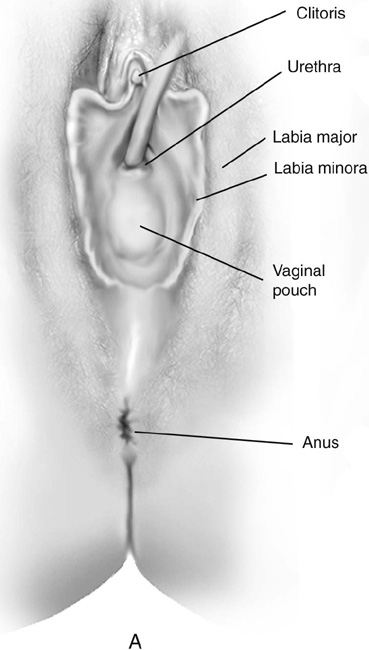
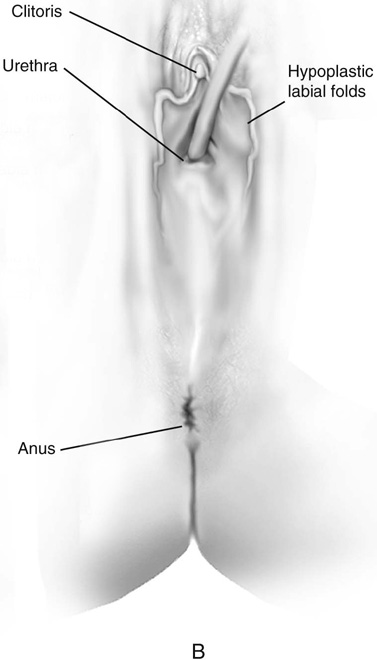
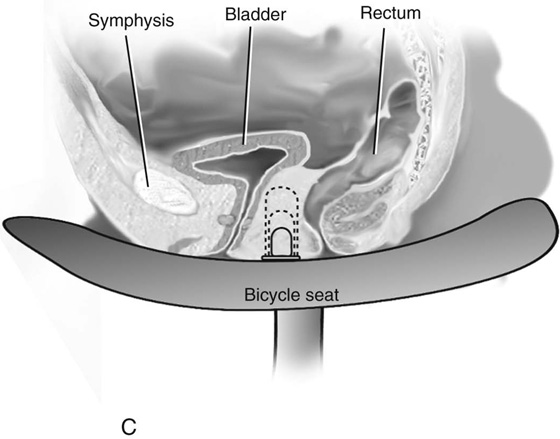
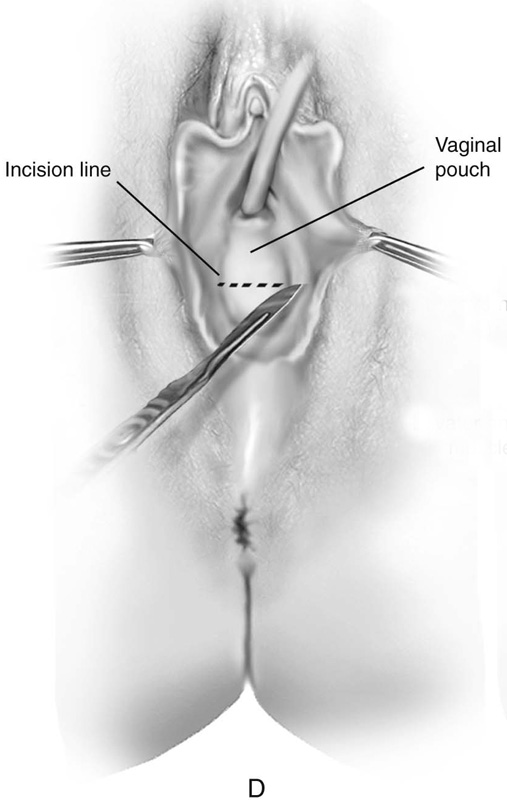
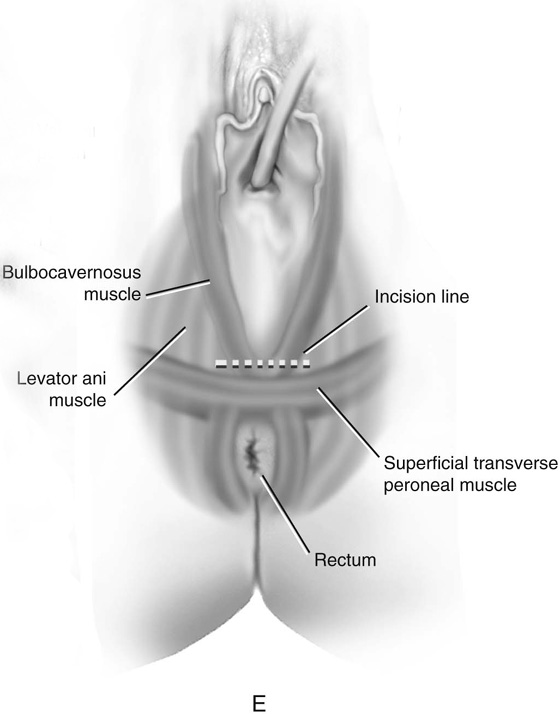
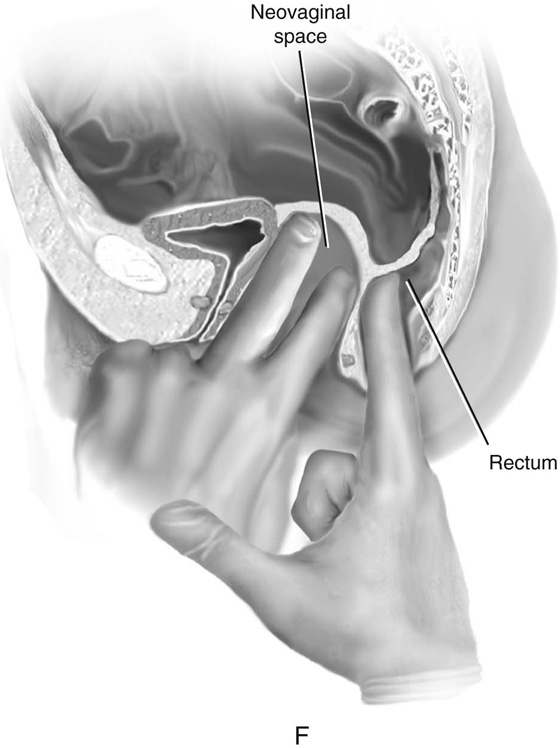
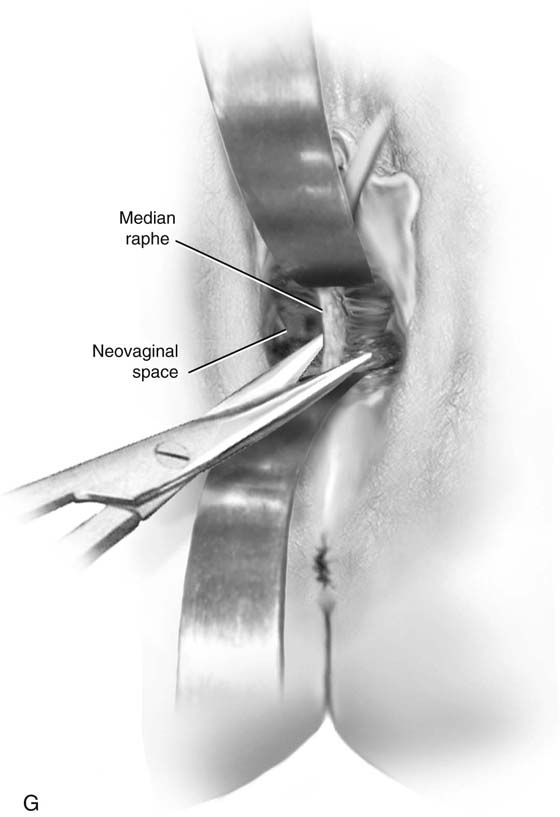
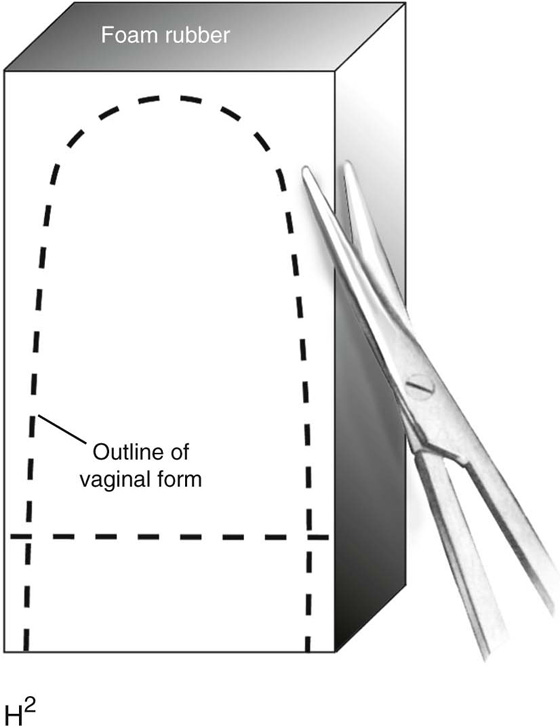
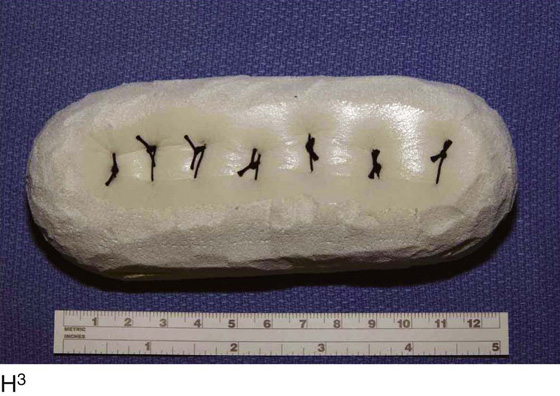
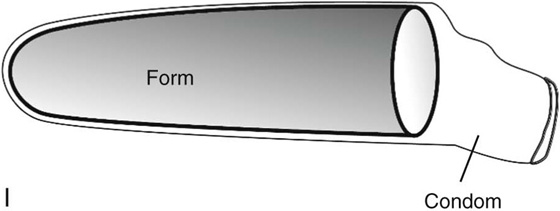
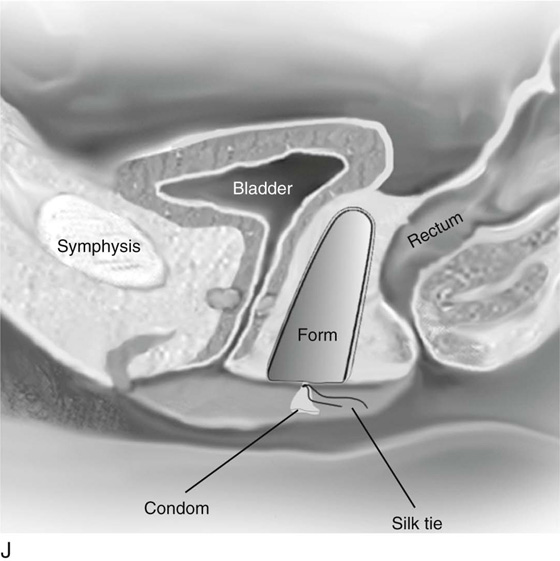
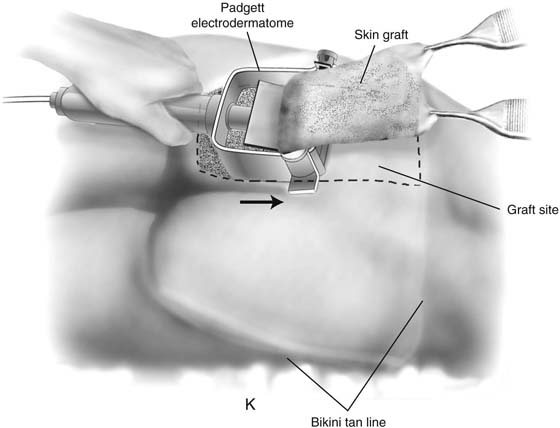
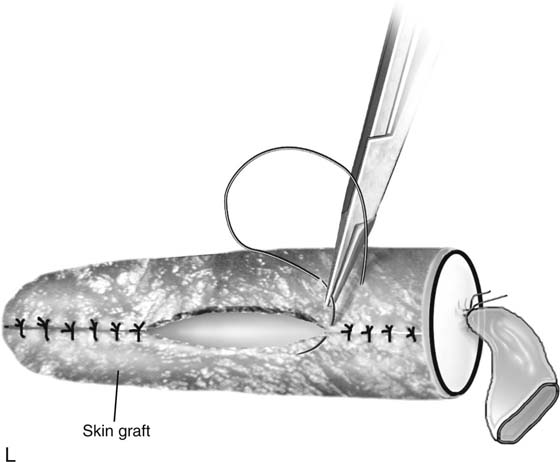
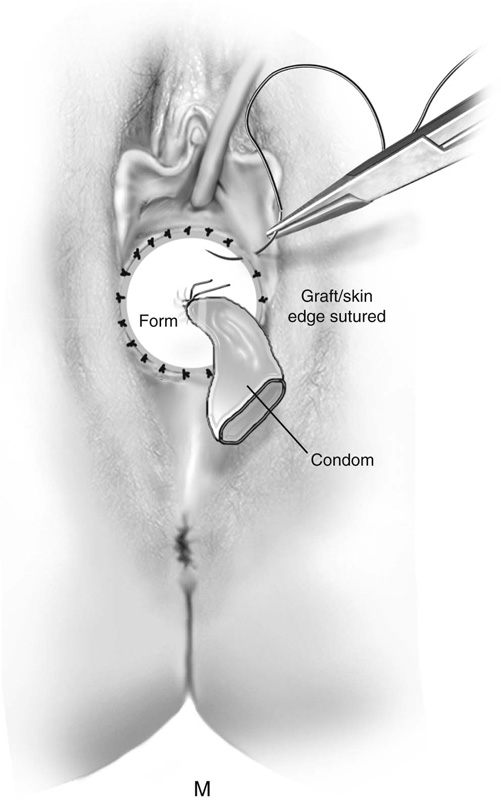
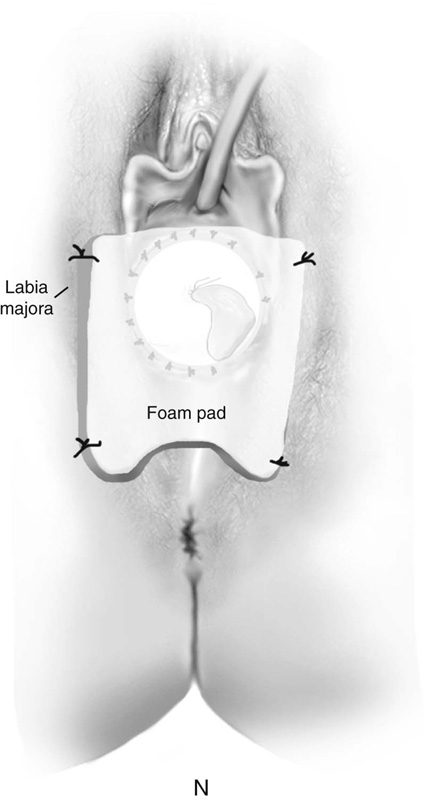
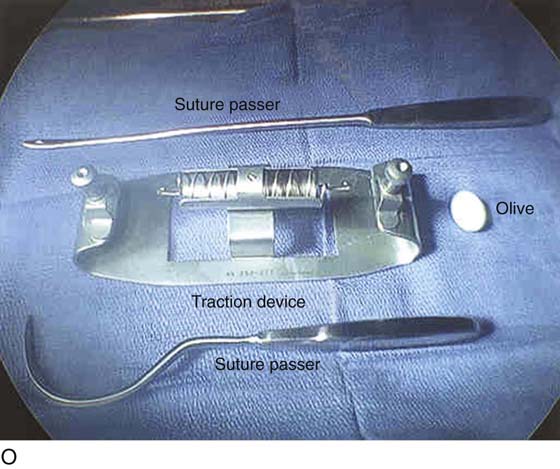
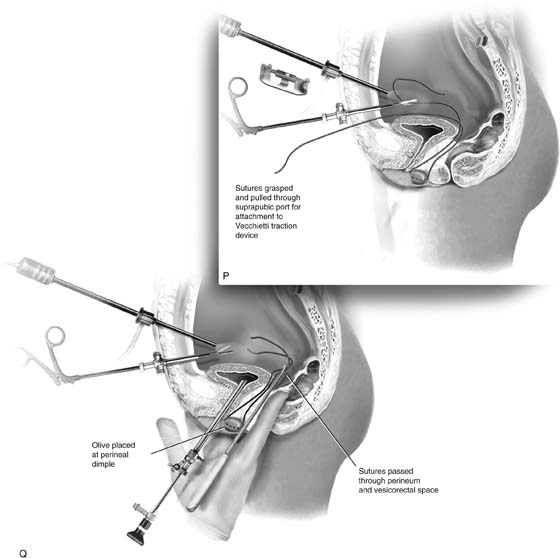
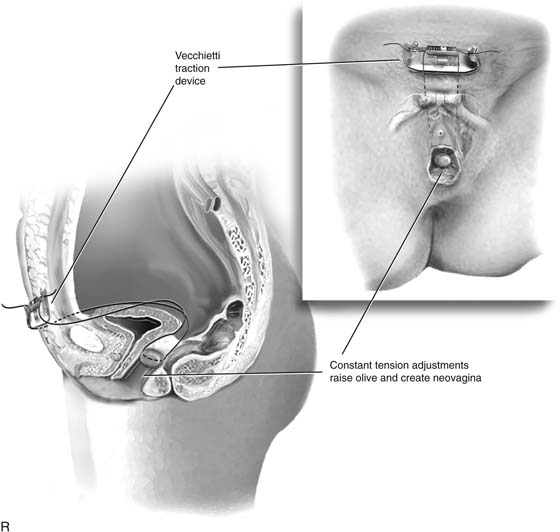
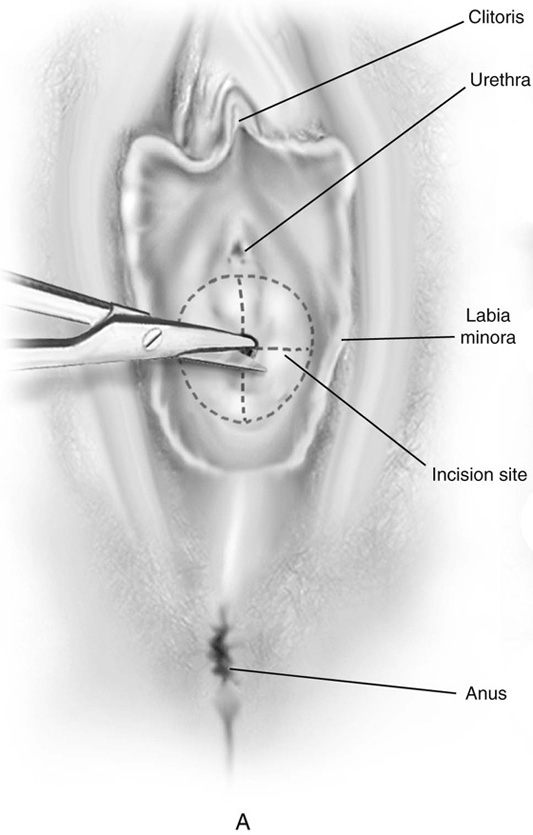
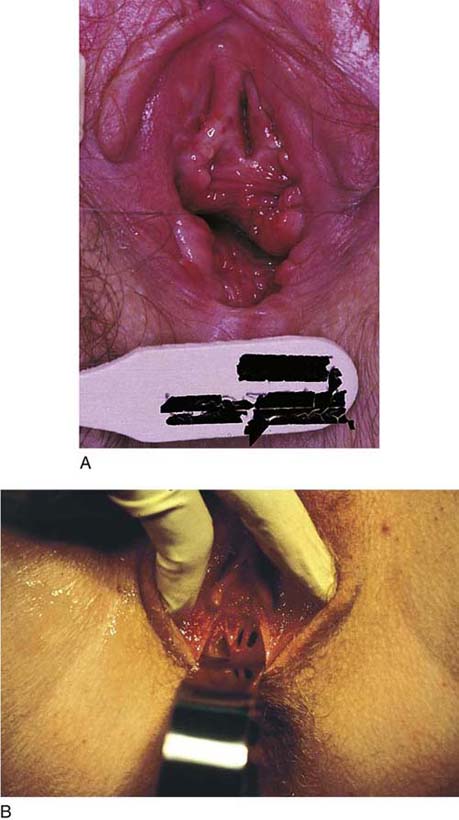
CHAPTER 61 John B. Gebhart A child or adolescent with an imperforate hymen presents with pain and a thin, translucent membrane distended by blood or mucus. An imperforate hymen is often treated in the operating suite with sedation or general anesthesia. First, an incision is made in the center of the membrane, and the blood and mucus are evacuated. The incision is extended transversely to the lateral margins of the obstructing membrane (Fig. 61–1A, B). Next, the membrane is divided anteriorly, then posteriorly, to complete a cruciate incision. Finally, the redundant avascular tissue is excised (Fig. 61–1C). Bleeding should be minimal following resection of the hymenal membrane. Pressure applied with a damp sponge will control most bleeding sites. If the resection has been carried out too far, and the bleeding cannot be controlled with a sparing application of Monsel’s solution (ferric subsulfate) or light pressure, then simple interrupted sutures of 3-0 polyglycolic acid should be placed. A continuous running simple suture should be avoided because this may cause constriction of the hymenal ring. The appropriate result is a capacious introitus that functionally permits comfortable coitus (Fig. 61–2A). Other developmental abnormalities of the hymen, including cribriform and septated hymens (Fig. 61–2B), may require surgical intervention. As with the aforementioned, the goal of the surgery is to create a nonconstricting, functional vaginal introitus. FIGURE 61–1 A. The incision is extended laterally into the hymenal membrane from 3 to 9 o’clock, then along the midline from 12 to 6 o’clock. B. Resection of the hymenal membrane is completed as the avascular quadrants are excised. C. The hymenal flaps have been resected, and the areas between 1 and 5 o’clock and between 11 and 7 o’clock have been sutured to the vestibular margin with interrupted 3-0 Vicryl sutures. FIGURE 61–2 A. Eight weeks after resection of the hymen. The introitus is widely open. The patient has been inserting a large vaginal form for 4 weeks. B. This young woman has a cribriform hymen. It is excised in a manner similar to the imperforate hymen (see Fig. 61–1A through C). Müllerian agenesis occurs once in approximately 4000 to 5000 female births. Typical findings of Rokitansky-Kuster-Hauser syndrome include a small vaginal pouch and a normal perineum (Fig. 61–3A). Vaginal agenesis may also occur in a male pseudohermaphrodite. Genital appearance varies depending on the underlying causes. Occasionally, a “flat” perineum is found (Fig. 61–3B). Vaginal dilation using the Ingram method is the primary approach used to prepare the vagina for intercourse when a vaginal pouch is present. A series of progressively wider and longer dilators are used (Fig. 61–3C). The patient is instructed to position the dilator against the perineum, and to apply her weight gradually onto a bicycle seat that is affixed to a stool. In a motivated patient, the vagina can be prepared for intercourse after a few weeks of dilation. More than 90% of women who comply with this regimen achieve anatomic and functional success. The McIndoe vaginoplasty is the primary surgical approach for vaginal agenesis when dilation is unsuccessful or is not possible. The patient must be physically and emotionally prepared for the surgery and must anticipate intercourse in the not too distant future. FIGURE 61–3 A. Müllerian agenesis. The perineum is normal. A small vaginal pouch is evident. B. A flat perineum, which may be found in a male pseudohermaphrodite. No vaginal pouch is present. Labial folds, if present, terminate near the urethral meatus. C. Vaginal dilation with graduated dilators. Using a bicycle seat, the patient slowly sits on the dilator. Pressure on the dilator from the body’s weight allows complete dilation within a few weeks. D. Initial transverse incision into the apex of the vaginal pouch in a woman with vaginal agenesis. The initial incision should be at least 3 to 4 cm. E. Initial transverse incision is made immediately anterior to the superficial transverse peroneal muscle in the patient with a flat perineum. Relationships among the urethra, labia, rectum, and underlying musculature are shown. F. Blunt dissection into the neovaginal space. Dissection is performed laterally, then medially. If the patient is 46XY, sharp resection of the prostate may be necessary to avoid damage to the rectal mucosa. Care is taken not to dissect too large an area near the peritoneum because herniation may occur. G. Retractors are placed into the neovaginal space. The median raphe, a thick band of connective tissue, is divided sharply. H. A 10 × 10 × 20-cm sterile block of soft foam rubber is shaped according to the outline. The base is cut to accommodate the vaginal depth. The cut end is saved and later is used to protect the neovagina. I. A sterile condom is placed over the shaped vaginal form. J. After the form and the condom have been compressed, they are placed into the neovaginal space and allowed to expand for approximately 1 minute. A 2-0 silk tie is then secured at the base of the condom, and the form is removed. A second condom is placed over the first condom, and the base tied with 2-0 silk. K. The patient is placed in a lateral position. The buttock is prepped and draped, then is coated with sterile mineral oil. A Padgett electrodermatome with a 10-cm-wide blade is used to harvest a 0.45-mm-thick graft 15 to 18 cm long inside the bikini (tan) line if possible. L. The edges of the graft are approximated around the form with interrupted vertical mattress sutures of 5-0 polyglycolic acid. The skin surface touches the form. M. The form and the covering graft are placed into the neovaginal space. The edges of the graft are sutured to the perineal skin with interrupted absorbable suture material, approximately 1 cm apart, to allow drainage. N. A foam pad is placed over the perineum and is secured into the labia minora with 0 silk suture. A gap is cut near the anus to avoid contamination of the pad during a bowel movement. O. Instruments required for the Vecchietti vaginoplasty include a 2.2 × 1.9-cm acrylic “olive,” an abdominal traction device, a long perineum suture passer, and an alligator-jaw needle passer. P. A #2 polyglycolic acid suture is passed through the olive, and both free ends of the suture are placed in a long needle passer. Q. A laparoscope is placed through the umbilicus, and a secondary port is inserted above the symphysis. Concurrent cystoscopy is performed, and one finger is placed into the rectum to identify puncture of the bladder or bowel. The long needle passer is inserted from the perineum into the peritoneal cavity under direct laparoscopic visualization. A suture passer is placed through the skin into the abdomen in the right lower quadrant, approximately 2 to 3 cm above the symphysis. One end of the suture is grasped and pulled through the skin. This procedure is repeated through the left lower quadrant, so that both ends of the suture are removed through the abdomen. R. The sutures are attached to the Vecchietti device, and traction is applied to allow downward movement of the olive of 1 cm with countertraction. Tension should be equal on both sides of the device. Within 7 to 9 days, a 10- to 12-cm vagina is created. First, a transverse incision is made at the apex of the vaginal pouch in the patient with müllerian agenesis (Fig. 61–3D). If the perineum is flat, a 3- to 4-cm incision is made in the posterior fourchette, anterior to the anal sphincter (Fig. 61–3E). The neovaginal space is bluntly dissected laterally, then toward the midline. One finger is placed in the rectum for guidance (Fig. 61–3F). Sharp dissection is necessary in the male pseudohermaphrodite if the prostate remnant is adherent to the rectum. A thick band of connective tissue between the bladder and rectum—the median raphe—is sharply divided near the neovaginal fornix (Fig. 61–3G
Congenital Vaginal Abnormalities
 Lesley L. Breech
Lesley L. Breech  Bradley S. Hurst
Bradley S. Hurst  John A. Rock
John A. Rock
Imperforate Hymen
Vaginal Agenesis

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


