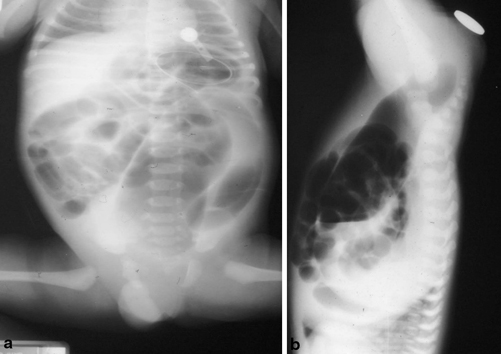
Fig. 30.1
A lateral photograph of a barium enema showing congenital rectal stenosis marked by arrows
Gupta and Sharma classified congenital rectal atresia into five types:
Type I: Rectal stenosis
Type II: Rectal atresia with a septal defect
Type III: Rectal atresia with a fibrous cord between the two atretic ends
Type IV: Rectal atresia with a gap
Type V: Multiple rectal atresia with stenosis (A) or without stenosis (B)
Clinical Features
Congenital rectal atresia in contrast to anorectal malformations is characterized by:
A normal-looking anus.
The anal canal and lower rectum are surrounded by a normally developed sphincter and hence a good functional postoperative outcome is expected.
Unlike other anorectal malformations , congenital rectal atresia usually has no associated fistula communication with the urogenital system.
Congenital rectal atresia commonly is an isolated malformation and without any other additional congenital anomalies.
Diagnosis
The diagnosis of congenital rectal atresia is clinical.
Patients usually present in the neonatal period with failure to pass meconium and abdominal distension (Fig. 30.2).
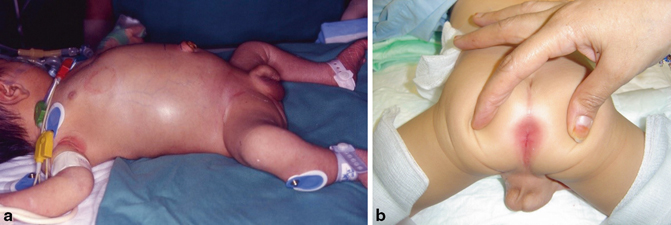
Fig. 30.2
Clinical photograph showing abdominal distension and a normal-looking anus in a patient with congenital rectal atresia
Clinically, there is a normal-looking anus.
Failure to pass a thermometer confirms the diagnosis.
Abdominal X-ray shows dilated bowel loops with no gas distally and an invertogram shows stoppage of the air in the distal rectum (Fig. 30.3).