Congenital Anomalies of The Skull Base
Susan I. Blaser, MD, FRCPC
DIFFERENTIAL DIAGNOSIS
Common
Internal Jugular Vein Asymmetry
Jugular Bulb Diverticulum
Chiari 1
Chiari 2
Neurofibromatosis Type 1
Less Common
Aberrant Internal Carotid Artery
Persistent Stapedial Artery
Carotid Artery, Sphenoid Migration
Agenesis Internal Carotid Artery
Rare but Important
Craniostenoses
4th Occipital Sclerotome Anomalies
Persistent Craniopharyngeal Canal
Medial Basal Canal (Basilaris Medianus)
Chiari 3
ESSENTIAL INFORMATION
Helpful Clues for Common Diagnoses
Internal Jugular Vein Asymmetry
Key facts: Right internal jugular vein (IJV) dominant in 68-75%
Left IJV commonly smaller than right
IJV asymmetry < in larger cranial vault
Imaging
Most commonly seen normal asymmetry: Right sigmoid sinus, jugular bulb, and IJV larger than left
Increased signal of left IJV due to compression of left brachiocephalic vein during respiratory cycle
Jugular Bulb Diverticulum
Key facts: Asymptomatic normal variant
Imaging
Coronal best: Bone CT, MRV, or T1 C+
“Pouch” projects from jugular bulb
High signal on MR may simulate mass
Chiari 1
Key facts: Mismatch between posterior fossa size and cerebellar tissue
Imaging
Low-lying pointed (not rounded) peg-like cerebellar tonsils
Tonsils project below (≥ 5 mm) OR are impacted in foramen magnum
4th occipital sclerotome anomalies in > 50% small occipital enchondral skull
small occipital enchondral skull
Chiari 2
Key facts
100% with neural tube closure defect
Imaging
Small bony posterior fossa
“Scalloped” petrous pyramid
“Notched” clivus
Low-lying tentorium/torcular
Large funnel-shaped foramen magnum
Neurofibromatosis Type 1
Key facts: Neurocutaneous disorder
Characterized by diffuse neurofibromas, intracranial hamartomas, benign and malignant neoplasms
Imaging
Progressive sphenoid wing dysplasia
Enlarged optic foramina and fissures
Foramen magnum and skull base defects
Helpful Clues for Less Common Diagnoses
Aberrant Internal Carotid Artery
Key facts: Displaced ICA courses through middle ear
Imaging
Enters posterior middle ear through enlarged inferior tympanic canaliculus
Courses anteriorly across cochlear promontory
Joins horizontal carotid canal through dehiscent carotid plate
Absent carotid foramen & vertical segment of petrous ICA
Look for associated persistent stapedial artery (PSA) in 30%
Persistent Stapedial Artery
Key facts
Embryologic stapedial artery persists
PSA becomes middle meningeal artery
Imaging
Enlarged CN7 canal
Small canaliculus leaving carotid canal at genu of vertical and horizontal petrous ICA
Absent ipsilateral foramen spinosum
Carotid Artery, Sphenoid Migration
Key facts: Seen in skull base syndromes involving enchondral bone
Achondroplasia, branchiootorenal syndrome, bicoronal synostoses (Apert, Pfeiffer, Crouzon)
Imaging
Medial migration of bony carotid artery walls at level of sphenoid
Agenesis Internal Carotid Artery
Key facts
Isolated or syndromic (PHACES, morning glory, Goldenhar, clefting syndromes)
Imaging
Absent or hypoplastic vertical and horizontal petrous portions of ICA
Helpful Clues for Rare Diagnoses
Craniostenoses
Key facts
Syndromic (fibroblastic growth factor, TWIST, and MSX2 mutations) + nonsyndromic premature osseous obliteration of cranial sutures
Imaging
Early fusion of occipital sutures surrounding foramen magnum
Enchondral skull base: Achondroplasia, syndromic bicoronal synostoses, kleeblattschädel
4th Occipital Sclerotome Anomalies
Synonym: Proatlas anomalies
Hypocentrum of 4th occipital sclerotome (OS) anterior clival tubercle
anterior clival tubercle
Centrum of 4th OS apical cap of dens and apical ligament
apical cap of dens and apical ligament
Ventral portion of neural component of 4th OS anterior margin of foramen magnum and occipital condyle
anterior margin of foramen magnum and occipital condyle
Caudal portion of neural component of 4th OS lateral atlantal masses and superior posterior arch of atlas
lateral atlantal masses and superior posterior arch of atlas
Imaging: 4th OSA finding
Short clivus and atlas assimilation
Craniovertebral bony anomalies
Persistent Craniopharyngeal Canal
Key facts
Look for associated canal atresia or stenosis, moyamoya, coloboma
Imaging
Small: Nonpituitary tissue containing remnant channel
Large: Contains pituitary gland or frank encephalocele or artery
Medial Basal Canal (Basilaris Medianus)
Key facts
Notochord remnant cephalic terminus
Imaging: Midline clivus
Posterior to sphenooccipital synchondrosis
Currarino types A-F denote completeness and location of defect
Tortuous canal may indent superior or inferior aspect of clivus
Chiari 3
Key facts: Intracranial Chiari 2 + meningoencephalocele
High cervical meningoencephalocele
Imaging
Occipital squama defect may involve upper cervical vertebrae
Bony features of Chiari 2 in addition
Image Gallery
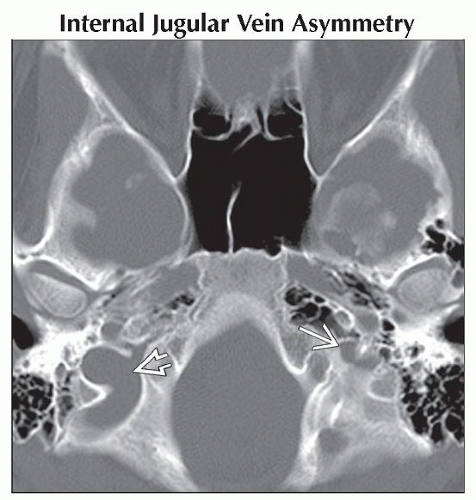 Axial bone CT demonstrates marked asymmetry with the jugular foramen on the right  larger than the small left jugular foramen larger than the small left jugular foramen  . . |
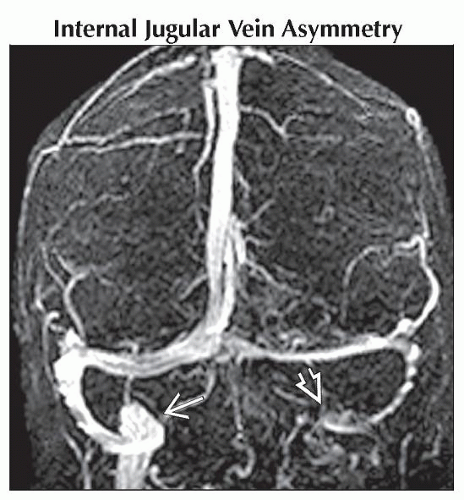 Coronal MRV in the same patient confirms marked asymmetry of the jugular veins. The left  tapers and is poorly visualized while the right tapers and is poorly visualized while the right  is normal in size. is normal in size. |
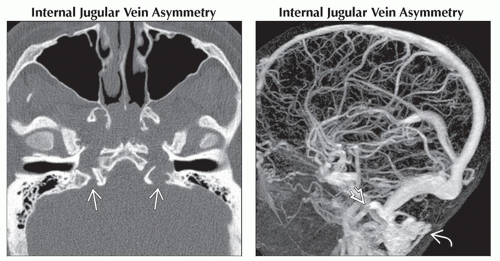 (Left) Axial bone CT in a teenager with achondroplasia shows asymmetry of the jugular foramina
 , both of which are stenosed. (Right) Sagittal MRV in a different patient with achondroplasia reveals severe restriction of the jugular vein , both of which are stenosed. (Right) Sagittal MRV in a different patient with achondroplasia reveals severe restriction of the jugular vein  at the level of the stenosed jugular foramina. There are excessive venous collaterals at the level of the stenosed jugular foramina. There are excessive venous collaterals  in the soft tissues of the neck. in the soft tissues of the neck.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|