Fig. 56.1
Clinical photograph showing the components of the cloacal extrophy
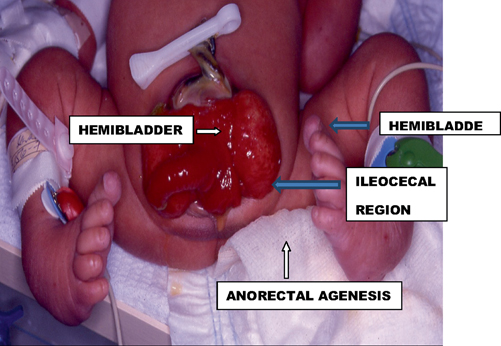
Fig. 56.2
Clinical photograph showing a classic cloacal extrophy
Cloacal extrophy, which is also called vesico-intestinal fissure, is one of the rare and complex malformations with a reported incidence between 1 in 200,000 and 1 in 400,000 live births.
Classically, cloacal extrophy consists of five components:
Omphalocele .
Extrophy of the two hemi bladders .
Lateral cecal fissure which presents between the two hemi bladders.
Imperforate anus .
Ambiguous genitalia .
Many other variants have also been described .
Embryology
The exact embryogenesis of cloacal extrophy is not known, and many theories have been suggested; however, no single theory can adequately explain all the abnormalities seen in cloacal extrophy .
The most accepted theory is that cloacal extrophy results from premature rupture of the cloacal membrane prior to caudal migration of the urorectal septum, and fusion of the genital tubercles.
Embryologically, the urorectal septum divides the cloaca after the fourth week of intra-uterine life into an anterior urogenital sinus and a posterior anorectal canal.
The cloacal membrane is invaded by lateral mesodermal folds at approximately 4 weeks of gestation.
It is postulated that if this mesodermal invasion does not occur, the infraumbilical cloacal membrane persists leading to poor lower abdominal wall development.
The cloacal membrane eventually ruptures but if this happens prior to the descent of the urorectal septum, which happens at 6–8 weeks of gestation, then cloacal extrophy results .
So cloacal extrophy occurs due to the failure of two concomitant mesodermal migrations. First, the urorectal septum fails to develop and divide the urogenital sinus from the rectum; second, the mesodermal proliferation forming the infraumbilical abdominal wall and genital tubercle fails to develop.
Failure of these two events to occur results in extrophy of both bladder and intestine.
Classically, cloacal extrophy is made up of omphalocele , extrophied ileocecal region of bowel, extrophied hemi bladders each with its ipsilateral ureter, and anorectal agenesis.
The pubic bones are widely separated, and spinal dysraphism is common in these patients .
Associated Anomalies
Cloacal extrophy is commonly associated with other anomalies including cardiovascular and central nervous system anomalies .
Omphalocele (70–90 %).
Vertebral anomalies (46 %).
Upper urinary tract (42 %). Upper urinary tract anomalies include pelvic kidney, horseshoe kidney, hypoplastic kidney, and solitary kidney.
Malrotation (30 %).
Lower extremity anomalies (30 %) (Fig. 56.3).

Fig. 56.3
Clinical photograph of a newborn with cloacal extrophy. Note also the bilateral talipes equinovarus
Double appendix (30 %).
Absent appendix (21 %).
Short small bowel (19 %).
Small bowel atresia (5 %).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


