Fig. 55.1
Contrast study showing a classic cloaca where the rectum, vagina, and urethra join together and open in a single perineal opening
Fig. 55.2
Diagrammatic representation of a cloaca showing the urethra, vagina, and rectum joining together in a common channel
The length of the common channel varies from 1 to 10 cm, with an average of approximately 3 cm (Fig. 55.3).
Fig. 55.3
a and b Diagrammatic representation of cloaca. Note the length of the common channel which is variable, ranging from 1 to 10 cm but commonly around 3 cm
It is important to correctly diagnose persistent cloaca in the neonatal period because 90 % of babies with this malformation have an associated urologic problem, and 40 % have hydrocolpos .
About 30 % of these patients have a hydrocolpos. The hydrocolpos may produce two important complications:
It may compress the trigone of the bladder, producing ureterovesical obstruction, megaureter, and hydronephrosis.
The hydrocolpos if left undrained may become infected, leading to a pyocolpos .
Approximately 40 % of these patients have a double Mullerian system consisting of two hemiuteri and two hemivaginas. This septation disorder may be partial or total and symmetric or asymmetric.
The urinary tract and the distended vagina may both need to be managed within the newborn period to avoid serious complications.
The goals of treatment include:
Early diagnosis
Immediate neonatal management
An anatomic reconstruction to achieve bowel and urinary control, as well as normal sexual function
Clinical Features
Persistent cloaca is a clinical diagnosis.
The presence of a single perineal orifice provides clinical evidence of persistent cloaca (Fig. 55.4).
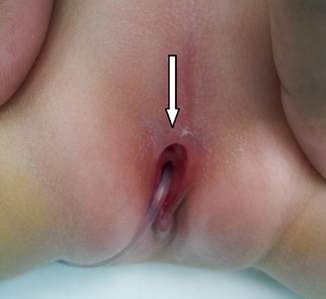
Fig. 55.4
Clinical photograph showing a single perineal opening in a patient with cloaca
The external genitalia often appear small.
Examination of the abdomen may reveal an abdominal mass (hydrocolpos).
The distended vagina is a common cause of an obstructed urinary tract because of its pressure on the trigone; therefore, once the vagina is decompressed, the urinary tract may no longer be obstructed. If the hydrocolpos is not drained during the newborn period, it can become infected forming pyocolpos .
A hemisacrum is almost always associated with a presacral mass, commonly teratomas, or anterior meningoceles.
The Currarino triad includes an anorectal malformation, a hemisacrum, and a presacral mass.
Associated Anomalies
Associated defects are common with cloaca.
Most vital to recognize are the urological abnormalities.
More than 80 % of all patients with a cloaca have an associated urogenital anomaly.
These include absent kidney, vesicoureteral reflux, horseshoe kidney, ectopic ureters, double ureters, hydronephrosis, and megaureters as a result of vesicoureteral reflux or ureterovesical obstruction.
A tethered spinal cord: an intravertebral fixation of the phylum terminale.
Patients with anorectal malformations and tethered cord have a worse functional prognosis regarding bowel and urinary function.
Sacrum and spine anomalies. The sacrum is the most frequently affected bony structure. Anomalies of the sacrum include hypodevelopment, sacral hemivertebrae, and hemisacra.
Hemivertebrae may also affect the lumbar and thoracic spine, leading to scoliosis.
Patients with cloaca may have spinal anomalies other than tethered cord, such as syringomyelia and myelomeningocele.
Investigations
Plain radiography of the spine can show spinal anomalies, such as spina bifida and spinal hemivertebrae.
Plain radiography of the sacrum in the anterior–posterior and lateral projections can reveal sacral anomalies, such as a hemisacrum and sacral hemivertebrae.
Abdominal ultrasonography to evaluate for urologic anomalies and a distended vagina (hydrocolpos).
Spinal ultrasonography in the first 3 months of life.
Magnetic resonance imaging (MRI) to evaluate the anomalies of the cloaca, the presence of tethered cord and sacrum and spine (Figs. 55.5 and 55.6).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


