Clinical Presentation of Respiratory Illness
Hans Pasterkamp
Respiratory illness in children usually presents with clinical symptoms and signs that offer important information for further diagnostic tests. The primary function of the respiratory system is to provide a supply of oxygen and removal of carbon dioxide, that is, adequate and adaptive gas exchange. Illness can disturb this function by affecting respiratory control, the respiratory pump, that is, chest cage and respiratory muscles, airways, and the pulmonary tissues. The many nonrespiratory functions of the lung include production and regulation of surfactant, defense against infections, participation in water and fluid balance, sieving of blood cells and emboli, and elimination of volatile substances. The clinical presentation of illness interfering with these functions is often related to the secondary effects on respiratory mechanics and gas exchange.
RESPIRATORY SCORES
Efforts to formalize the assessment of clinical signs in respiratory illness for estimation of disease severity have resulted in numerous clinical scores, for example, for croup,1 bronchiolitis and pneumonia,2 and for asthma.3,4 Clinical signs as the basis of these scores include tachypnea, visibly increased respiratory effort, for example, retractions and use of accessory muscles, reduced breath sound intensity (often referred to as “air entry”), wheezing, relative duration of expiration, cyanosis, and mental status.
RESPIRATORY RATE
The number of breaths per minute is counted by observing chest and abdominal movements or by listening to breaths with a stethoscope. Respiratory rates established by auscultation may be slightly higher than those by observation, particularly when placement of the stethoscope on the chest stimulates the child. Children have higher respiratory rates during wakefulness than during sleep. The range of respiratory rates in a healthy child is wide but narrows when a higher breathing rate is maintained during respiratory illness. Breathing rates are related to age and weight, showing an exponential decrease with increasing age and body mass. Age specific normative data have been established for infants and toddlers5 and for older children6 (Fig. 505-1). Fever and respiratory disease can increase the respiratory rate. In young febrile children tachypnea, that is, a respiratory rate faster than normal, is an important predictive sign for pneumonia when the respiratory rate per minute exceeds 59 in those under 6 months of age, 52 between 6 and 11 months, and 42 between 1 and 2 years.7 Observer agreement on tachypnea is generally good.
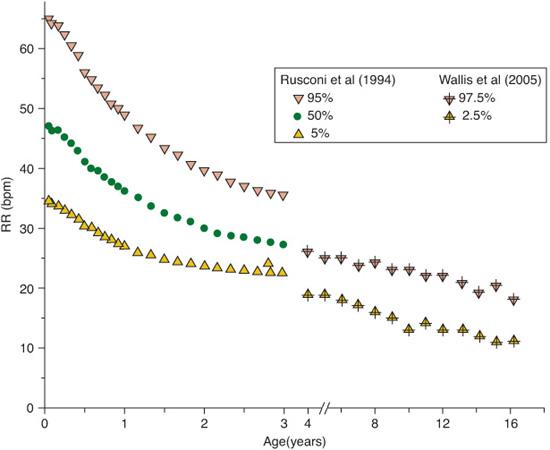
FIGURE 505-1. Normal range of respiratory rates during wakefulness. (Data from Rusconi FM, Castagneto L, Gagliardi G, et al. 1994. Reference values for respiratory rate in the first 3 years of life. Pediatrics. 1994;94:350-355. Wallis LA, Healy M, Undy MB, Maconochie I. Age related reference ranges for respiration rate and heart rate from 4 to 16 years. Arch Dis Child. 2005;90:1117-1121.)
RETRACTIONS, ACCESSORY MUSCLE USE, AND PULSUS PARADOXUS
Increased resistance to airflow can lead to inspiratory retractions of the more compliant parts of the chest. These are most easily visible in young children because of their lower mass and greater compliance of the chest wall. Retractions can be sub- and intercostal, and above the thoracic inlet, that is, supraclavicular and suprasternal. The severity of airway obstruction may be reflected by the extent to which all of these areas are involved. Palpation of the trachea in children with suprasternal retractions may detect a tug, that is, a posterior downward movement. Deviation of the trachea from midline can be a sign of unilateral lung disease. Chronic retractions may cause changes in the configuration of the chest over time, for example, development of secondary pectus excavatum or “funnel chest,” or the appearance of a Harrison sulcus, a groove at the lower rib cage at the level of the diaphragmatic insertion.
With increased respiratory effort, secondary or accessory respiratory muscles are increasingly used. Most visible are the contractions of the sternocleidomastoid and scalene muscles that augment rib cage volume. Pectoralis major, trapezius, and abdominal muscles (rectus, oblique, and transverse abdominis) are also involved to stabilize the chest and abdominal walls. Nasal flaring, that is, the contraction of the alae nasi, widens the nasal aperture and reduces flow resistance. Observer agreement on retractions is only fair.
Pulsus paradoxus refers to an exaggerated (ie, more than 10 mmHg) decrease of systolic blood pressure during inspiration. It is a hallmark finding in cardiac tamponade and it is often used in the assessment of acute asthma, at least in adults. However, the value of this sign as an indicator of the severity of airway obstruction is controversial8 and the measurement can be particularly difficult in children. It remains to be seen whether the plethysmo-graphic pulse wave on oximetry may offer improved measurements of pulsus paradoxus.
WORK OF BREATHING
It has become widely accepted to report increased work of breathing as a clinical presentation of respiratory illness. However, the work of breathing is determined by physiologic measurement of intrathoracic pressure swings inside the esophagus and is expressed in Joules, where one Joule is the energy required to move 1 L of gas through a pressure gradient of 10 cm H2O.9 The clinical description of the work of breathing is based on a gestalt, a pattern of physical phenomena that integrates to a functional assessment. Usually this will include increased visible respiratory effort, that is, increased respiratory rate, and signs related to increased flow resistance, including retractions, and use of accessory muscles.
In healthy subjects, the amount of energy dedicated to breathing is small (ie, less than 3% of total body oxygen consumption). Obese individuals spend more energy on breathing than those of normal weight, even at rest. Several but not all subjects with chronic lung disease show an increase in resting energy expenditure. Some of this is related to an increased work of breathing but other factors, including relatively reduced energy intake, also contribute. Reasons for increased caloric cost of breathing in respiratory illness include not only increased resistance to air flow (eg, in airway obstruction), or decreased pulmonary compliance (eg, in atelectasis and restrictive lung diseases), but also restrictive chest wall conditions (eg, in severe scoliosis, or increased chest wall distortion in infants with respiratory illness). The result of these changes becomes apparent in many children with chronic respiratory illness as failure to thrive. In adults with chronic obstructive pulmonary syndrome, the term pulmonary cachexia has been used.10
RESPIRATORY SOUNDS
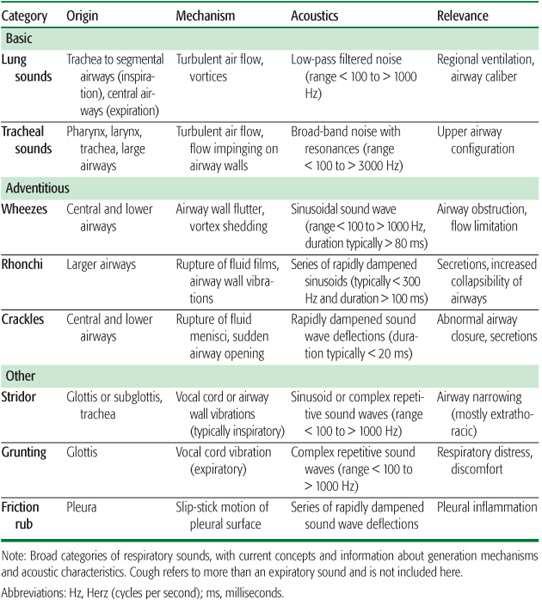
Respiratory sounds fall into the broad categories of normal or basic breath sounds, and of abnormal or adventitious breath sounds (Table 505-1). Basic breath sounds arise from turbulent flow of air in large airways, with inspiratory sounds originating more peripherally than expiratory sounds. Depending on the site of auscultation (eg, at the neck, close to large airways, or more peripherally on the chest), there will be a loss of sound energy from absorption in lung tissues and chest wall. Thus, tracheal sounds are comparatively loud and quite similar during inspiration and expiration while lung sounds at the chest are more muffled and have relatively less intensity during expiration.11
Basic breath sounds can provide information about the distribution of ventilation. Decreased loudness of breath sounds may point to reduced ventilation of the underlying lung, for example, in the presence of atelectasis or consolidation, or the collection of fluid or air in the pleural space. An overall reduction of the loudness of breath sounds may occur when the lungs are overinflated, for example, in asthma or emphysema. Stiffening of the airway walls during bronchial constriction may also reduce the transmission of breath sounds. Reduced “air entry” in children with acute asthma may be a misinterpreted sign because blood gas analysis will often show normal or even reduced carbon dioxide levels, indicating normal or even increased alveolar ventilation.
Table 505-1. Respiratory Sounds
Normal anatomic asymmetries of the intrathoracic structures can explain some naturally occurring asymmetries of basic respiratory sounds. Expiratory sounds tend to be slightly louder over the anterior right upper lung than on the left while inspiratory sounds are often slightly louder over the posterior left lung compared to the right. Careful comparison over corresponding areas of both lungs may detect bronchial breathing (ie, abnormally increased loudness of expiratory sounds) closer in character to tracheal sounds. This bronchial breathing may be present over areas of reduced air content, for example, over a consolidated or atelectatic lung. A dull note on percussion may suggest reduced air content of the underlying structures, for example, when atelectasis or consolidation reduce the air content and thus the acoustic impedance change between chest wall and parenchyma. Conversely, the percussion note may be hyperresonant when the air content is increased, for example, in emphysema or pneumothorax. However, compared with auscultation, percussion has even greater observer variability and lower predictive values.
Adventitious, or abnormal breath sounds fall into the two subcategories of musical or tonal wheezes, sometimes referred to as “continuous” because of their relatively longer duration, and nonmusical, popping crackles, also referred to as “discontinuous” because of their very brief duration. The mechanisms behind these two types of adventitious sounds are quite different and therefore point to different disease processes.
Wheezes arise from the vibration or flutter of airway walls when there is excess energy for generating air flow. This can occur when flow becomes limited in narrowed airways, that is, when an increase in driving pressure does not generate more air flow.12 Most healthy subjects can produce wheezes with maximum effort because flow is normally limited during the later period of forced expiration. Therefore, asking for maximum forced expiration to find wheezing is not useful because such forced expiratory wheezes are not specific to disease. On the other hand, shallow breathing may not generate the force necessary to cause airway wall flutter and wheezes, even in the presence of obstructive airway disease. Deeper than normal breathing should therefore be encouraged to detect wheezing during chest auscultation.
Inspiratory wheezing is quite common during acute airway obstruction, for example, in asthma. It is important to distinguish inspira-tory wheezing from stridor. The latter is also a sound of somewhat musical character, typically arising from extrathoracic airway obstruction, and often heard without the aid of a stethoscope. Stridor tends to be louder and is more prominent at the neck and distributed over the entire chest while inspiratory wheezing is not as loud, often more prominent over particular regions of the chest. As an adventitious respiratory sound with somewhat musical character, wheezing is classified by its pitch. High-pitched wheezing is typical for airflow obstruction because of airway constriction, for example, in asthma and bronchiolitis. Low-pitched wheezes include rhonchi. These share some acoustic similarity with snoring and are common in the presence of increased airway secretions. Frequently, such “secretion sounds” will change after spontaneous or voluntary cough. Parents and caregivers may use other terms to describe wheezing, and their characterization of whistles, purrs, and rattles may have prognostic value regarding the child’s risk for developing asthma.13
Crackles are another subcategory of adventitious respiratory sounds. They originate from the rupture of fluid films, for example, when air moves through secretion filled airways, and also from the sudden opening of closed airways. These mechanisms cause local stress and relaxation of the airway wall and surrounding parenchyma that translates into pressure waves that reach the chest surface as sound and can be heard with a stethoscope. The duration of a single crackle is usually too short to be heard as a tone but there are differences in the frequency content of the crackle sound wave that lead to different audible crackle characteristics. Fine crackles have higher frequency but are often not as loud as coarse crackles. To hear them best, slower deep breaths should be encouraged to avoid the generation of loud normal lung sounds that may mask their presence. Fine crackles leave the impression that they originate closer to the ear than coarse crackles, and recent acoustic studies with arrays of microphones lend support to this assumption.14
The two types of crackles also point to different underlying respiratory pathologies. Fine crackles are often heard in diseases that are not very common in children, that is, in diffuse infiltrative pulmonary processes (eg, asbestosis and sarcoidosis). Fine crackles occur with the sudden opening of airways and are useful indicators of disease in children with interstitial pneumonia. In adults, posturally induced fine crackles (those that occur only in the supine position, for example) can be signs of cardiac failure, but this has not been described in children. Showers of fine crackles, for example, in interstitial pulmonary fibrosis, have been referred to as Velcro rales. However, use of the word rale is being discouraged because of its ambiguity. Rene Laennec, the inventor of the stethoscope, used rale to describe a wide range of adventitious sounds.
Coarse crackles are a frequent finding in children with respiratory disease. They are typically louder than fine crackles and their sound waves have a lower frequency. Coarse crackles are common in airway diseases that are accompanied by increased airway secretions, for example, bronchitis and bronchiolitis. Coarse crackles are also often present in children with pneumonia and in congestive heart failure. Coarse crackles in rapid sequence can assume a snoring, rhonchus-like character. This is often noticed in children with increased oropharyngeal secretions, for example, in patients with swallowing dysfunction. The gurgling crackly sounds are often audible without a stethoscope and may be very loud at the chest surface. Typically these secretions sounds change or disappear after suctioning.
CYANOSIS AND OTHER SIGNS OF HYPOXEMIA
Cyanosis refers to bluish or purplish coloration of skin and mucous membranes, caused by an increased proportion of deoxygenated hemoglobin in the circulation. The level of deoxygenated hemoglobin has to reach approximately 50 g/L in capillary blood, or 34 g/L in arterial blood, for cyanosis to occur. Significant hypoxia may therefore present without cyanosis in patients with anemia. Furthermore, agreement among observers regarding cyanosis is not perfect, and factors such as room lighting or skin pigmentation can contribute to the variation.
Usually the lips and fingers are assessed for the presence of cyanosis. Peripheral cyanosis of fingers and toes can be present without arterial hypoxemia when oxygen extraction in the capillary bed is increased due to sluggish circulation, for example, with cold-induced vasoconstriction or with decreased perfusion pressures. Central cyanosis, for example, of the lips, is more reliable as an indicator of arterial hypoxemia. However, bluish coloration around the mouth, or perioral cyanosis, in the absence of cyanosis of the lips, is peripheral in nature.
Certain dyshemoglobins, particularly met-hemoglobin and, rarely, sulfhemoglobin, can cause cyanosis. Cyanotic skin coloration, most obvious on mucous membranes, can occur when methemoglobin levels reaches 15 g/L in patients without anemia (normally, methemoglobin constitutes less than 1% of total hemoglobin). Cyanosis is neither sensitive nor specific as a sign of arterial hypoxemia. Pulse oximetry has been considered as the fifth vital sign, but this objective measurement of oxygenation is also affected by dyshemoglobins. A discrepancy between oxygen saturation measured by pulse oximetry and calculated from arterial blood gas analysis should lead to a search for dyshemoglobins.
A reduction of arterial oxygen levels increases the respiratory drive. The sensation of an increased drive in healthy subjects will not usually occur before arterial PO2 decreases below 55 mmHg. In patients with asthma the sensation of increased respiratory resistance may be actually reduced by hypoxia. The subjective sensation of acute breathlessness and “air hunger” is well recognized as an important clinical presentation of serious respiratory or cardiac illness. Dyspnea describes a subjective experience of breathing discomfort that is comprised of qualitatively distinct sensations that vary in intensity. The experience derives from interactions among multiple physiological, psychological, social, and environmental factors, and may induce secondary physiologic and behavioral responses.15 Several clinical scoring systems have been developed to quantify breathing discomfort in adult patients with chronic obstructive lung disease. Labored breathing can develop during heavy exercise in healthy subjects. Older children and adolescents can express their experience of breathlessness during physical exercise similar to adults. However, there are few tools to quantify dyspnea in the pediatric population.
In pediatric practice, dyspnea is often assumed to be present, based on the impression of visible respiratory effort and anxiety in children who are too young or otherwise unable to report their sensation of breathlessness. In these situations it may be useful to describe the signs of respiratory distress, for example, tachypnea, retractions, accessory muscle use, and restlessness, rather than to imply a subjective sensation.
DIGITAL CLUBBING
Respiratory illness can present with clubbing of the digits, that is, with enlargement of the terminal segment of fingers and/or toes. In children, the most common respiratory diseases that present with clubbing are bronchiectasis due to cystic fibrosis or other causes, chronic lung infection, and pulmonary abscess. The most common nonrespiratory diseases presenting with clubbing are congenital heart disease, infectious endocarditis, hepatic cirrhosis, and inflammatory bowel disease. Rarely, clubbing can be idiopathic. Digital clubbing may present during the first half year after birth and it can disappear after the underlying cause has been removed, for example, after lung or liver transplantation.
The mechanisms responsible for digital clubbing are not entirely clear but genetic factors, the direct effect of tissue hypoxia, or circulating vasodilators that escape metabolism in diseased lungs, as well as vagus mediated neural effects have all been postulated. More recently, platelet precursors that are not fragmented into platelets on their passage through the pulmonary circulation have been invoked as a cause. These precursors may get trapped in peripheral vessels where they can release platelet-derived and vascular endothelial growth factors that promote vascularity.16 Clubbing is usually painless and often not recognized by the patient.
Morphologically, the nail bed in clubbing shows an increased caliber and number of blood vessels, also primitive fibroblasts and an increased number of lymphocytes and eosinophils.17 On physical examination, inspection of the nail-fold angles and palpation of the base of the nail bed are used. Viewed in profile, the normal angle that the nail plate makes with the adjacent skin fold is 150 to 170 degrees, whereas the hyponychial angle (from nail plate to distal nail) is between 178 and 192 degrees. Schamroth described a sign where the rhombus that is normally seen when the dorsal surfaces of the right and left index finger are placed against each other disappears in the presence of clubbing. A simple and validated test of nail fold angles at the bed side is the phalangeal depth ratio. With clubbing, the depth of the finger at the proximal nail fold exceeds the depth of the distal interphalangeal joint. Clubbing can be one of the most precisely identified physical signs of respiratory illness when it is fully developed, but observer agreement on clubbing in the early stages is only modest.
CHEST PAIN
(See Chapter 486.)
COUGH
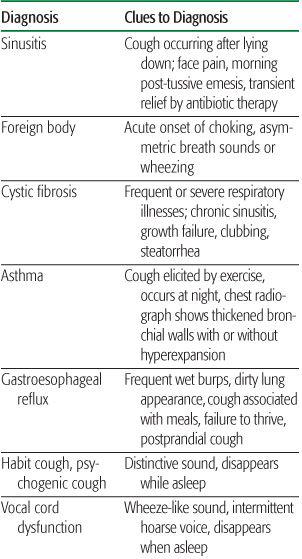
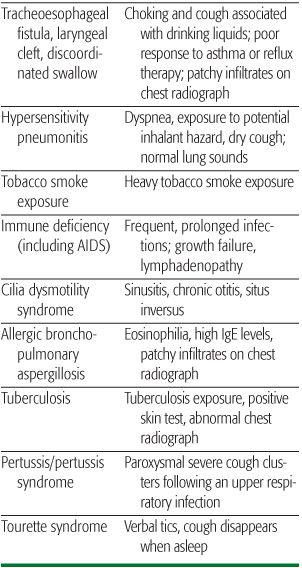
A cough is a voluntary or involuntary explosive expiration. After a deep inspiration, the glottis is closed and the expiratory muscles contract, compressing the lung and raising intrapulmonary pressure above the atmospheric pressure. The glottis then opens, and gas is expelled at a rapid rate. The cough reflex is initiated by the stimulation of subepithelial mechanoreceptors in the trachea, bronchi, and interstitium. Cough receptors may be activated by dust, chemicals, inflammation, mucus, airway distortion, or rapid changes in airway volume. A series of coughs that is difficult to stop is called a paroxysm and is common in pertussis, viral infections, cystic fibrosis, gastroesophageal reflux, and asthma. During paroxysms of coughing, central venous blood pressure rises, cerebral venous blood flow falls, and intracranial pressure increases. This may produce signs of cerebral hypertension such as headache, vomiting, conjunctival hemorrhage, or blurred vision. When foreign bodies or excess mucus is present, coughing is essential to eliminate the obstruction or facilitate mucociliary clearance. The high intrathoracic pressures that are created during active expiration, however, can collapse and obstruct the unstable airways of young infants or patients with bronchiectasis. Parents of children with chronic cough often seek medical attention as persistent symptoms are often uncomfortable (or even harmful), and may be associated with chest pain or poor sleep quality. Chronic cough may also result in pulmonary air leaks or rib fracture. The differential diagnosis of chronic cough includes chronic sinusitis, gastroesophageal reflux, asthma, and other chronic lung diseases including cystic fibrosis and bronchiectasis. A diagnostic approach to chronic cough is presented in Table 505-2.
Table 505-2. Differential Diagnosis of Cough
HEMOPTYSIS
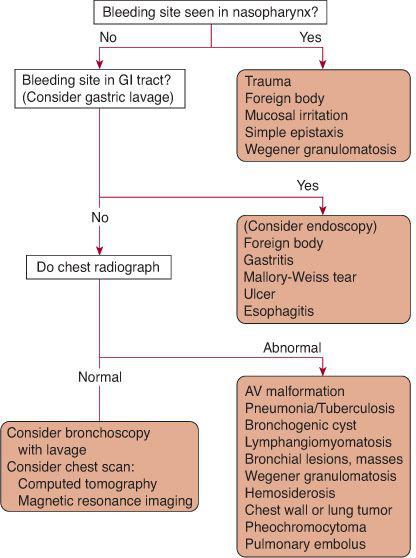
Hemoptysis is defined as bleeding that originates from the airway or the lung parenchyma but is observed in the upper airway or in expectorated secretions, typically by coughing. Acute hemoptysis results from inflammation or trauma to the nasopharynx, larynx, or esophagus. Epistaxis and hematemesis also may be confused with hemoptysis, and the nasopharynx and gastrointestinal tract must be considered in the evaluation of a patient suspected to have hemoptysis. Intermittent hemoptysis is common in chronic conditions such as cystic fibrosis and bronchiectasis, in which there is chronic infection. Significant bleeding into lung parenchyma (eg, that seen in pulmonary hemosiderosis or pulmonary vasculitis syndromes) may not cause obvious hemoptysis because much of the blood is swallowed or retained in the interstitial space or alveoli. Pulmonary arteriovenous malformations anywhere in the respiratory tract may also cause hemoptysis.
Some authors advocate considering whether the patient has had a localizing or nonlocalizing radiologic study. For example, if the radiologic evaluation reveals a mass in one lung, then the diagnostic algorithm should be directed to the differential diagnosis of the mass and the appropriate diagnostic approach as opposed to determining the source of bleeding. However, nonlocalizable hemoptysis occurs when there is no localized lesion on chest radiologic studies. In this case, flexible fiberoptic bronchoscopy can be useful in evaluating patients with unexplained hemoptysis. Either the site of bleeding may be directly visualized, or analysis of lavage may reveal hemosiderin-laden macrophages, thus establishing the diagnosis of pulmonary hemorrhage when the bleeding site cannot be seen. A diagnostic approach to hemoptysis is shown in Figure 505-2.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


