Age
Gender
Number of siblings
Birth order
Length of pregnancy
Obstetric presentation
Presence or absence of difficulty with delivery
Birth weight
As active or less active than siblings in utero
Developmental motor milestones
Family history of orthopedic, neuromuscular, renal, or endocrine disorders
The clinician should determine at what age the deformity was first noticed. Intoeing which does not appear until approximately age 2 years is usually due to resolution of the physiologic external rotation contracture of the infant hip, unmasking the persistent tibial torsion and/or proximal femoral antetorsion.
Does it seem to be getting better, worse, or remaining the same? For example, bowing of the lower extremities is a normal consequence of the in utero position and will resolve spontaneously (Fig. 2.1); the gradual improvement in the bowing helps establish the diagnosis and rules out Blount disease or metabolic bone disease, two conditions that require a more extensive work-up and treatment.
Fig. 2.1
The development of the tibiofemoral angle in children during growth; the standard deviation is ±8°. Adapted with permission from Zaleske DJ. Metabolic and endocrine disorders. In: Morrissy RT, Weinstein SL, editors. Lovell and Winter’s Pediatric orthopedics, 4th edition. Philadelphia: Lippincott-Raven; 1996 [58]
Is there any history of fractures, lower extremity injuries, bone or soft-tissue infections, or previous surgery? The development of an angular deformity or leg length discrepancy following a fracture or infection may indicate a partial or complete injury to the growth plate.
Is there any family history of orthopedic, neuromuscular, renal, or endocrine disorders? Is there any family history of short stature? A family history of hypophosphatemic rickets, Charcot–Marie–Tooth disease, or kidney failure with renal rickets should alert the clinician to conditions that may be inherited.
Physical Examination
Although many children who present for evaluation have an obvious diagnosis, one must always perform an examination that includes at least the vital signs (height, weight, body mass index (BMI)), upper extremities, spine and trunk, neurological, gait, and lower extremities. Although the gait and lower extremity exam will be the most detailed, the other components are necessary and can be performed quite rapidly.
Vital Signs
Height and weight should be measured at the office visit instead of asking the family to furnish this information because parents often are quite inaccurate with their child’s stated height and weight [5]. The BMI is a proxy for adiposity and can be calculated from the formula
 The percentile for age-related Z score should be determined from charts available from the Centers for Disease Control (http://www.cdc.gov/growthcharts/clinical_charts.htm). Very large age-related Z scores may indicate a condition associated with obesity such as Blount disease or Prader–Willi syndrome. Very low Z scores may indicate malnutrition, malabsorption, chronic metabolic disease, or skeletal dysplasia.
The percentile for age-related Z score should be determined from charts available from the Centers for Disease Control (http://www.cdc.gov/growthcharts/clinical_charts.htm). Very large age-related Z scores may indicate a condition associated with obesity such as Blount disease or Prader–Willi syndrome. Very low Z scores may indicate malnutrition, malabsorption, chronic metabolic disease, or skeletal dysplasia.
Upper Extremity
An abnormal carrying angle of the elbow, especially if symmetric, may indicate a skeletal dysplasia. Joint laxity with excessive motion, such as hyperextension of the elbows or interphalangeal joints, may indicate a connective tissue disorder. Palpable metaphyseal enlargements may indicate a rachitic disorder or multiple hereditary exostoses.
Spine and Trunk
The rib cage should be palpated for a rachitic rosary: swellings at the costochondral junction are indicative of a rachitic disorder. Screening for scoliosis is performed by checking for thoracic and/or lumbar asymmetry with forward bending.
Neurologic
A quick but quite sensitive screening battery for the detection of neurological disease affecting the lower extremity can be done in children and adolescents of walking age by having them walk on their heels in dorsiflexion, on their toes (metatarsal heads) in equinus, and hop on one leg at a time. To perform these maneuvers, the child utilizes quadriceps (L2, L3, L4), hip extensors (L5, S1, S2), hip abductors (L5, S1), ankle plantar flexors (L5, S1, S2), and ankle dorsiflexors (L4, L5). If there is a high level of suspicion for the presence of a neurological abnormality, a more detailed exam must be done, including searching for pathologic primitive reflexes.
Gait
The examiner should watch the child walk. Sometimes children walk in a certain pattern as instructed by their parents when aware that the physician is watching. Thus, it is helpful to watch the child walk from the waiting area to the exam room when he or she is unaware of being examined. One should watch the child walk both with shoes and barefoot because shoes may hide dynamic conditions such as searching toes or dynamic forefoot adduction, two conditions attributed to contraction of the abductor hallucis creating a concave medial border of the foot during gait.
Foot Progression Angle
The foot progression angle is the angle between the axis of the foot and the line of progression, with intoeing expressed as negative values and out-toeing expressed as positive values [2, 6]. A study of gait in 160 children (up to 14 years of age) concluded that the normal angle of gait was approximately 10° external at all ages with a slight decrease after age 7 [7] (Fig. 2.2). The mean foot progression angle is a positive value (external rotation) throughout childhood and adulthood. However, negative values (internal rotation) are considered normal (within two standard deviations) throughout childhood and early teens [2]. Etiologies contributing to an internal rotation gait include excessive acetabular anteversion, excessive femoral anteversion, internal tibial torsion, metatarsus adductus (MTA), and searching toe. Etiologies contributing to an external rotation gait include acetabular retroversion, physiologic external rotation contracture of the hips, femoral retroversion, external tibial torsion, and positional calcaneal valgus. These conditions may be additive or may compensate for each other [8].
Fig. 2.2
The foot progression angle changes with age. The normal range is very broad. Adapted from [4]
Short Leg Gait
A child with a limb length inequality may walk with the foot and ankle in equinus or with an abductor lurch on the short side during stance phase of gait. Other compensatory mechanisms for a short lower extremity include flexing the contralateral knee and/or dropping the ipsilateral hemipelvis.
Equinus
Unilateral equinus is often seen in patients with hemiparetic cerebral palsy, some unilateral foot deformities, and limb length inequality. An equinus position in stance phase of gait is the most common compensating mechanism for a limb length inequality. Bilateral equinus may indicate idiopathic toe walking or neuromuscular disease, such as cerebral palsy or muscular dystrophy.
Trendelenburg Sign
The child should stand on one foot while the clinician observes for the pelvis dropping toward the opposite side. Normally, the child should not allow the pelvis to drop for at least 15 s. A positive sign with the pelvis dropping indicates abnormal ipsilateral femoral pelvis anatomy (such as acetabular dysplasia, dislocated or subluxated femoral head, proximal femoral deformity) or abductor weakness.
One must compare the gait appearance to the findings on the exam table. For example, forefoot adduction during gait but not in the nonweight-bearing position is frequently due to the normal phasic activity of the toe flexors and tibialis posterior muscles in stance phase; these muscles insert medial to the midline of the foot and may act as forefoot adductors during gait. The great toe may abduct during stance phase of gait. This condition, called wandering or atavistic toe, is attributed to the phasic activity of the abductor hallucis muscle [4, 8].
Lower Extremities
Supine Exam
A general assessment of the lower extremities in the supine position on the exam table includes evaluation of the limb lengths, as seen by the levels of the plantar aspects of both feet and the measurement of the distance from the anterior superior iliac spine to the medial malleoli. Any asymmetry of thigh circumference, leg circumference, or foot length should also be noted. If a discrepancy in limb lengths is noted, the patient should be examined with blocks underneath the short leg to determine when the pelvis is level. This method has been shown to be the most reliable clinical measurement for leg length discrepancy, although the studies were done in adults [9, 10].
Varus (bow legs) and valgus (knock knees) angulations at the knee are measured with a goniometer on the anterior aspect of the extremity with the patellas forward. Measuring the distance between the knees or medial malleoli to quantify varus or valgus is less reliable; there may be variability due to adiposity, size of the patient’s legs or thighs, and limb torsion. Bowing of the lower extremities is normal until age 2 years. Persistent varus after age 2 years or excessive valgus may be a manifestation of a traumatic, congenital, developmental, or metabolic disease [11–16] (Table 2.2).
Table 2.2
Etiologies of lower extremity deformity
Varus |
Traumatic |
Proximal tibial physeal injury (may also be valgus) |
Congenital |
Tibial hemimelia |
Developmental |
Achondroplasia |
Campomelic dysplasia |
Congenital pseudarthrosis of tibia |
Hypochondroplasia |
Metaphyseal chondrodysplasia (Schmid, Jansen, Spahr types) |
Neurofibromatosis |
Ollier disease (multiple enchondromatosis) (may also be valgus) |
Osteogenesis imperfecta (may also be valgus) |
Multiple epiphyseal dysplasia (may also be valgus) |
Multiple hereditary exostosis (may also be valgus) |
Spondyloepiphyseal dysplasia |
Thanatophoric dysplasia |
Tibia vara (Blount disease) |
Metabolic |
Vitamin D-deficient rickets |
Hypophosphatemic rickets |
Valgus |
Traumatic |
Proximal tibial physeal injury (may also be varus) |
Proximal tibial metaphyseal fracture sequela (Cozen phenomenon) |
Congenital |
Congenital deficiency of femur |
Posteromedial bowing of tibia |
Fibular hemimelia |
Developmental |
Ellis-van Creveld dysplasia |
Metatropic dysplasia |
Morquio syndrome |
Multiple hereditary exostosis |
Multiple epiphyseal dysplasia (may also be varus) |
Metabolic |
Chronic renal failure |
Although radiographs can distinguish between normal physiologic bowing of infancy and rare conditions requiring intervention, routine radiographic screening and referral are not cost effective and expose children to unnecessary radiation [11, 17]. The cover-up test is a useful screening to assess the alignment of the upper part of the lower leg in children presenting with bow legs between the ages of 1 and 3 years [17]. The lower extremity is positioned with the patella forward and the lower leg and foot are covered by the examiner’s hand. A positive test (bowing in the upper tibia) or neutral test (a straight thigh–upper leg axis) is an indication for radiographic evaluation. A negative test (slight valgus at the upper tibia) indicates physiologic bowing. A positive cover-up test has a high sensitivity; a negative cover-up test has a high specificity and negative predictive value [17] (Fig. 2.3).

Fig. 2.3
Cover-up test of the proximal left tibia. (a) A varus or neutral alignment is a positive test. (b) A valgus alignment is a negative test. Courtesy of Jon R. Davids, M.D.
Limb length is measured from the anterior superior iliac spine to the medial malleolus with a tape measure (Fig. 2.4). If a limb length discrepancy is found, a cooperative child should stand with blocks underneath the short extremity to determine what size lift will level the pelvis. Older children and adolescents should be asked to report what amount of elevation for the short extremity makes them feel level and well corrected. Patients with long-standing limb length discrepancies usually report that they feel well corrected when the blocks under the foot undercompensate for the discrepancy because they have become partially accustomed to the discrepancy. Standing on blocks is more accurate (greater reliability) and also incorporates the foot and pelvis, unlike the supine tape measure technique [18].

Fig. 2.4
The lower extremity length is measured from the anterior superior iliac spine to the medial malleolus with a metal tape measure
The lower extremity may appear short if an ipsilateral hip or knee flexion contracture or an adduction contracture of the hip is present while standing; likewise the extremity may appear long if an ipsilateral hip abduction contracture is present. Any difference in the size of the foot should also be noted. Foot size discrepancies are seen in hemihypertrophy, neurological disease, and vascular disease.
To determine if a discrepancy is due to a femoral or tibial difference, the child should sit on the exam table with the hips and knees flexed 90°, the patellas forward, and feet unsupported. If there is a femoral discrepancy, the knees will appear to be at a different level when viewed from above; if a tibial discrepancy is present, the feet will be at different levels when viewed from the front. In many cases, there is a discrepancy in both segments.
Prone Exam
The prone exam (with measurement of hip rotation, thigh–foot angle, and foot alignment) is an excellent qualitative assessment of rotational conditions affecting the lower extremity.
Femoral Version and Antetorsion
Hip rotation in the prone position is the net result of soft-tissue rotation contracture, acetabular version, and femoral version (anteversion or retroversion). Axial rotation of the acetabulum and femur within two standard deviations of the age-related mean value is considered normal and is termed version; values outside two standard deviations are termed torsion [4].
Hip rotation should be evaluated with the child prone and the hip extended because the hip functions largely in extension during normal gait. Also, hip flexion in the supine position relaxes the anterior hip capsule, causing an inaccurate assessment of rotation [16]. The child should be positioned prone, with one hand lightly on the pelvic area to detect what degree of rotation rocks the pelvis off the table. The knee is flexed 90°. The leg serves as an indicator of rotation, measuring its angulation from vertical [6] (Fig. 2.5). Normal age-dependent values for internal rotation and external rotation have been published [2, 4, 6] (Fig. 2.6).
Fig. 2.5
Assessment of hip rotation with 45° internal and 45° external rotation. With kind permission from Springer Science+Business Media: Paley D. Principles of deformity correction. Berlin, Heidelberg; 2002 [23]
Fig. 2.6
Values for hip rotation and anteversion, according to age (horizontal axis). Adapted from [4]
The normal hip arc of motion, the sum of internal and external rotations, is approximately 80°–100° [6, 19], with greater external rotation than internal rotation until the age of 3–5 years [4, 7, 20]. Due to the in utero position, infants often have an external rotation contracture of the soft tissues around the hip at birth that gradually resolves by age 18 months. This soft-tissue contracture can mask the underlying femoral antetorsion. This physiologic soft-tissue contracture is at its maximum value at birth and is the usual etiology for external rotation exceeding internal rotation until age 18–24 months [20]. Femoral antetorsion (abnormally high value for anteversion) manifests as an increase in hip internal rotation and a decrease in external rotation without affecting the total rotational arc. It is the most common cause of intoeing in early childhood, tends to occur more in girls, and is usually symmetric [8]. As the physiologic soft-tissue external rotation contracture resolves, internal rotation of the hip increases [8]. For this reason, parents often report that their child became more pigeon toed or walked with more intoeing at age 18–24 months.
Other etiologies of excessive external rotation include acetabular retroversion, as seen in Down syndrome [21], and femoral retroversion, as seen in slipped capital femoral epiphysis (SCFE), coxa vara, and proximal focal femoral deficiency (PFFD). Jacquemier et al. defined normal age-related values of acetabular version in a study of 143 children between ages 1 and 15 years [22]. Because the significance of abnormal acetabular version in infants and children is unknown at present, radiographic studies are rarely done to measure acetabular version; therefore, the true prevalence of acetabular retroversion in children is largely unknown. Coxa vara and PFFD usually exhibit a decreased arc of rotation (less than 90°) on the prone exam and are detectable on the supine exam as decreased hip abduction or, in unilateral cases, a limb length discrepancy.
A severe valgus deformity of the proximal tibia will cause an apparent increase in external rotation and decrease in internal rotation without affecting the total rotational arc, whereas a severe varus deformity will cause an apparent increase in internal rotation and decrease in external rotation (Fig. 2.7), but this is rarely significant in an evaluation of pediatric patients [23].
Fig. 2.7
A 30° valgus deformity of the proximal tibia results in an incorrect assessment of 75° external rotation (instead of 45°) and 15° internal rotation (instead of 45°). Adapted with permission from Lippincott Williams and Wilkins/Wolters Kluwer Health; Jacquemier M, Jouve JL, Bollini G, Panuel M, Migliani R. Acetabular anteversion in children. J Pediatr Orthop. 1992;12(3): 373–5 [22]
In conclusion, in the vast majority of cases of infants with more external rotation than internal rotation in the prone position with the gradual diminution of the discrepancy, the etiology is a physiologic external rotation contracture of infancy (PERCI) especially between birth and age 18 months. Increased internal rotation compared to external rotation is often indicative of femoral antetorsion.
In most cases, a qualitative clinical examination, based on comparing hip internal and external rotations, is sufficient without a quantitative imaging study. Imaging to quantify femoral version is indicated only if hip rotation is significantly asymmetrical, operative correction is planned, or version must be measured to determine the cause of failure of prior surgical procedure around the hip [4]. Most authors conclude that femoral anteversion is not harmful [8, 16, 24], although it may require surgical correction when associated with excessive external tibial torsion [4, 19], abnormal acetabular version [19, 25], neuromuscular disease [26], or developmental dysplasia of the hip (DDH) [25, 26].
Tibial Torsion
Tibial version is normal in children and, by definition, torsion is abnormal [2, 4]. However, the term tibial torsion will be used here to include both normal and abnormal values because of its common usage. The thigh–foot angle (TFA) is the angle formed by the longitudinal axis of the thigh with the longitudinal axis of the hindfoot. The TFA is measured in the prone position with the hip in neutral rotation, the knee in 90° flexion, and the ankle and foot in neutral dorsiflexion (Fig. 2.8). Although this assessment of the TFA is a qualitative diagnostic test for tibial torsion, a goniometer may be used for quantifying this angle and to compare on subsequent exams. External tibial torsion is diagnosed and quantified with a positive value if the foot is externally rotated on the leg; internal tibial torsion is diagnosed and quantified with a negative value if the foot is internally rotated on the leg.
Fig. 2.8
The thigh–foot angle (TFA) assesses tibial torsion. (a) External tibial torsion. (b) Internal tibial torsion. Adapted with kind permission from Springer Science+Business Media: Paley D. Principles of deformity correction. Berlin, Heidelberg; 2002 [23]
The TFA averages 5° internal (range 30° to +20°) in infants and averages 10° external (range 5° to +30°) by the age of 8 years [8]. Katz reported internal tibial torsion on the left side more frequently than the right in a series of 54 females and 45 males [27]. Normal age-related values have been published [2, 4]. Staheli et al. assessed the normal range and interobserver error. They found that the normal range, defined as within two standard deviations, is quite large, with a standard deviation of 4.9°–8.9°. They concluded that values from 5° to 30° were within the range of normal during childhood [2].
Tibial torsion can also be diagnosed and quantified by determining the transmalleolar axis (TMA). With the child in the sitting position with the hip flexed and patella facing forward, the angle between the TMA and the coronal plane is assessed [28, 29]. Measurement can also be done in the prone position by locating the transmalleolar axis, drawing a line perpendicular to this axis, and then measuring the angle this line forms with the long axis of the thigh. The result obtained by the TMA method yields a value a few degrees greater than the TFA method, but the TFA is easier to measure [2]. While the TMA method measures only the tibial and fibular rotations, the TFA method is also affected by hindfoot abnormalities. More accurate quantification by diagnostic imaging is rarely indicated unless corrective osteotomies are being planned. Since internal tibial torsion is a normal condition in infants and children and normally resolves without treatment, corrective osteotomies are rarely indicated.
Axial Foot Deformities
The alignment of the foot as a possible cause of intoeing or out-toeing can also be assessed with the child in the prone position. The examiner should note whether the medial and lateral borders of the foot are straight (Fig. 2.9). The heel bisector line, a line through the midline axis of the hindfoot and forefoot, passes through the second web space in a normal foot. Originally described by taking a photocopy of the foot, a method of making a permanent paper document, the child is held in a weight-bearing position on the photocopy machine. The method can also be used while examining the child prone [30]. If the heel bisector line passes lateral to the second web space, the forefoot is adducted (MTA). If the line passes medial to the second web space, valgus is present. A concave medial border of the midfoot also indicates MTA. If MTA is present, the hindfoot can then be held with one hand while the examiner’s other hand abducts the forefoot to determine whether the MTA is rigid or supple. A normal foot should be flexible and exhibit slight forefoot abduction with gentle manipulation.
Fig. 2.9
The heel bisector line passes through the second web space in the normal foot (10A) and lateral to the second web space in metatarsus adductus. Adapted with permission from Smith JT, Bleck EE, Gamble JG, Rinsky LA, Pena T. Simple method of documenting metatarsus adductus. J Pediatr Orthop. 1991;11(5):679–80 [30]
Diagnostic Imaging
Whether to do imaging studies after a history and physical exam often presents a dilemma. The expense and radiation exposure with imaging should be avoided if the diagnosis is obvious from the history and physical exam and the imaging will not affect the decision making. Any limb length discrepancy, asymmetric angular deformity, or angulation outside the range of normal for age requires a full-length standing anterior–posterior image of both extremities to quantify the angular deformities and/or limb length discrepancy. Davids et al. noted that routine radiographic screening of children with bowed legs is not cost effective and exposes them to unnecessary radiation and recommended using the cover-up test to screen children between ages 1 and 3 years. Children with a negative cover-up test do not require radiography [17]. Guidelines for performing imaging studies for rotational conditions are less clear. Children with rotational components more than two standard deviations outside the mean, short stature (less than twenty-fifth percentile), asymmetric hip abduction or rotation, a positive Trendelenburg sign, marked limb asymmetry in length or alignment, or discomfort during gentle range of motion of the lower extremity should be considered for diagnostic imaging. A pelvic radiograph including a lateral view may be needed to rule out disorders such as hip dysplasia and SCFE in a child presenting with a gait abnormality and pertinent history and clinical exam [8].
Assessment of Limb Length
Several techniques have been developed for the measurement of limb length discrepancies, including orthoroentgenograms [31], slit scanography [32], standing teleroentgenograms [23, 33], scanograms [34], computerized tomography (CT) scanogram [35], and ultrasound [36]. The ideal method should be accurate, readily available in the physician’s office, and technically easy. Its cost and radiation dosage should be low. Its measurements should exhibit good reproducibility (Table 2.3).
Table 2.3
Comparison of methods for assessing leg length discrepancya
Methods | Reliabilityb | Accuracyb | Magnification | Approximate radiation exposure (mrads) | Approximate charges (US dollars) | Radiographic deformity analysis | Incorporation of height of the foot and pelvis | Typical availability in the USA | Weight bearing |
|---|---|---|---|---|---|---|---|---|---|
Clinical | |||||||||
Supine tape measure—“Real” (ASAS to malleolus) | + | + | None | None | Office visit | Not applicable | No | Yes | No |
Supine tape measure—“Apparent” (umbilicus to malleolus) | + | + | None | None | Office visit | Not applicable | Partial | Yes | No |
Standing blocks | ++ | + | None | None | Office visit | Not applicable | Yes | Yes | Yes |
Imaging | |||||||||
Teleoroentgenogram | ++++ | +++ | ~5% | 42 | $95c | Yes | Yes | Varies | Yes |
Orthoroentgenogram | +++ | +++ | Minimal | 200 | $110c | No | No | Varies | No |
Scanogram | ++++ | +++ | Minimal | 200 | $110c | No | No | Varies | No |
Computed radiography | ++++ | +++ | Varies with technique (scanogram vs. teleoroentgenogram) | Varies with technique, less exposure than standard radiography | $137d | Varies with technique (scanogram vs. teleoroentgenogram) | Varies with technique | Varies | Varies with technique (scanogram vs. teleoroentgenogram) |
Microdose digital radiography | +++ | ++++ | None | 2 | $75c | Yes | Yes | No | Yes |
Ultrasound | +++ | ++ | None | None | Not reported | No | No | No | Yes |
CT scan (digital localization image) | ++++ | ++++ | Minimal | 60 | $60c | Minimal | None | Varies | No |
MRI | ++++ | +++ | Minimal | None | Not reported | Not reported | Not reported | No | No |
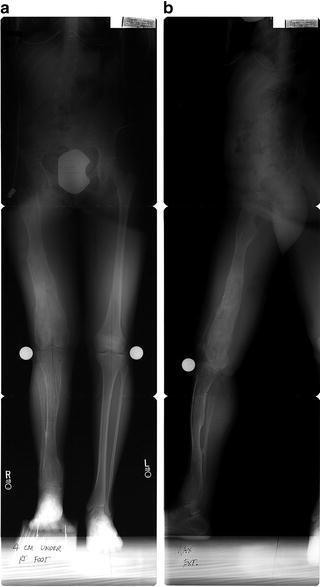
A single-exposure standing teleroentgenogram taken with the patella straight forward with a distance of 10 ft between the beam source and the film offers the best combination of benefits and fewest shortcomings (Fig. 2.10). It can easily be performed. Radiation exposure is greater than the CT scanogram technique [35] but less than the three-view scanogram [33]. With the advent of digital radiography and picture archiving and communication systems (PACS), the image can be manipulated to minimize radiation exposure and film storage is not a problem. By using a large distance between the beam source and the film, parallax and magnification (of up to 5 %) are introduced. Measurements can be made directly with a ruler or with computer software [33]. The image is made in the weight-bearing position. Angular deformities and bone pathology that may contribute to angular deformity and length discrepancy such as osteochondromas, enchondromas, or malunited fractures are detectable (see Table 2.2). The contribution of each segment (pelvis, femur, tibia, and foot) can also be quantified. Intraobserver and interobserver measurement reliability is excellent with a teleroentgenogram [34].
Fig. 2.10
A single-exposure standing full-length radiograph with patella forward is used to evaluate limb length and deformity. Adapted with kind permission from Springer Science+Business Media: Paley D. Principles of deformity correction. Berlin, Heidelberg, 2002 [23]
A standardized radiographic technique avoids distortion and magnification due to divergence of the X-ray beam and is reproducible so that serial radiographs can be compared. A cassette with a variable grid to include the hip, knee, and ankle is used. The cassette measures 132.5 × 38.5 cm for larger patients and 94.5 × 38.5 cm for smaller children. The beam is centered at the knee with the beam source at least 10 ft from the cassette. Correct patient positioning requires patellas straight forward for the anteroposterior (AP) view and 90° orthogonal to the AP position for the lateral view. The knees should be in full extension, with the body weight distributed equally on both feet. If there is a leg length discrepancy, a block is placed under the shorter extremity to level the pelvis and to keep the knee extended with the weight equally distributed on both feet. In severely obese children or in the presence of severe angular deformity, it may be necessary to perform separate AP radiographs of the two lower extremities. A magnification standard, such as a 30 mm ball bearing, can be affixed to the extremity at the main site of interest or at the knee when assessing leg length. The ball bearing should be positioned at the level of the bone, the same distance from the cassette as the bone. This technique quantifies magnification, which is usually about 5 % [33]. The ball bearing or another magnification marker must be affixed to the extremity at the level of the bone, not directly on the cassette (Fig. 2.11a, b). Placing a ruler with radiopaque graduations on the cassette may not accurately quantify magnification because the ruler is closer to the film than the bone.