Child Abuse
Eva Ilse Rubio, MD
DIFFERENTIAL DIAGNOSIS
Common
Long Bone Fractures
Posterior, Lateral, Anterior Rib Fractures
Skull Fractures
Classic Metaphyseal Lesion
Solid Organ Lacerations
Inflicted Head Injury
Mimics of Child Abuse
Physiologic Periosteal Reaction (Mimic)
Nutritional Deficiency (Mimic)
Leukemic Lines (Mimic)
Birth Injuries (Mimic)
Infection (Mimic)
Osteogenesis Imperfecta (Mimic)
Menkes Syndrome (Mimic)
Less Common
Small Bone Fractures
Spinous Process Fractures
Scapular Fractures
Sternal Fractures
Vertebral Compression Fractures
Bowel Injury
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Age of child
Posterior rib fractures and intracranial injures more common in children < 1 year
Solid organ injury/blunt trauma more common at toddler age and older
Clinical presentation
Ranges from fussy/failure to thrive to frankly obtunded
Clinicians may detect inconsistent or implausible stories explaining injuries
Suspicious bruising patterns or soft tissue injuries
American College of Radiology Guidelines for Skeletal Survey
Dedicated AP views each of humeri, forearms, femurs, tibia/fibula, hands, feet
AP chest, AP abdomen
Lateral views of cervical, thoracic, lumbar spine
AP and lateral views of skull
Additional orthogonal views should be obtained of any suspected abnormality
Consider bilateral oblique rib views
“Babygram” images are inadequate
Follow-up skeletal survey performed 10-12 days after initial study is useful to detect fractures not initially seen, confirm equivocal findings
Helpful Clues for Common Diagnoses
Long Bone Fractures
Femur, humerus most common
Common but nonspecific injury
May be innocent fractures once children are mobile/toddling
Metatarsal/metacarpal fractures
Often buckled appearance, can be subtle
Posterior, Lateral, Anterior Rib Fractures
More common on left
May be subtle if minimally displaced, or acute without callus formation
Oblique views may increase detection
Skull Fractures
Common but nonspecific injury
Features that raise suspicion
Complex, displaced fractures
Crossing suture lines
Classic Metaphyseal Lesion
Accepted mechanism is shear injury through primary spongiosa of distal metaphysis due to grabbing, twisting
Common locations
Tibia, femur, humerus
Solid Organ Lacerations
Liver lacerations/contusions
Linear or branching, low-attenuation, intraparenchymal foci on CT
CT bone windows may reveal additional rib fractures overlying organ injury
Splenic lacerations/contusions
Linear or branching, low-attenuation, intraparenchymal foci on CT
Adrenal laceration/hematoma
Usually globular abnormality
High attenuation on CT if acute; low attenuation if subacute/chronic
Inflicted Head Injury
Subdural hematoma
Fluid collection overlying brain convexity, layering along tentorium and interhemispheric falx
Swirling low attenuation within high attenuation fluid may indicate active bleeding or dural injury with CSF leak
Interhemispheric hematoma increases suspicion for inflicted trauma
Subarachnoid hemorrhage
Wispy/linear high density following sulci
Anoxic injury
Early: Ill-defined, low-attenuation areas
Late: Progressively low-attenuating parenchyma, loss of gray-white matter differentiation, sulcal effacement
Mimics of Child Abuse
Physiologic Periosteal Reaction (Mimic)
Typically seen ages 1-6 months
Often symmetric but not exclusively
Appearance: Thin, smooth, diaphyseal
Nutritional Deficiency (Mimic)
Children with liver failure, TPN dependency, short gut syndrome
Rib and extremity fractures may be seen from normal patient handling
Leukemic Lines (Mimic)
Usually in older age group; neonatal leukemia very rare, associated with hepatosplenomegaly and chromosomal abnormalities
Expect symmetric manifestation
Birth Injuries (Mimic)
Most common: Clavicle, humerus fractures; subdural hematomas
Timing/manner of delivery important
Infection (Mimic)
Osteomyelitis, TORCH infections, especially syphilis
Osteogenesis Imperfecta (Mimic)
Appearance of bones ranges from near normal to osteopenic and dysmorphic
Menkes Syndrome (Mimic)
Intracranial parenchymal volume loss, hemorrhages, and metaphyseal lesions can be mistaken for abuse
X-linked disorder
Helpful Clues for Less Common Diagnoses
Small Bone Fractures
Buckle fractures of metatarsals, metacarpals
Spinous Process Fractures
Avulsion fractures of spinous process tips uncommon but highly specific for abuse
Scapular Fractures
Fractures of acromion, scapular body uncommon but highly specific for abuse
Sternal Fractures
Associated with blunt trauma
Consider vascular/cardiac injury
Vertebral Compression Fractures
Thoracolumbar compression fractures occur with axial loading force
Bowel Injury
Duodenum
Hematoma protruding as intraluminal mass or intramural lesion
Perforation: Look for retroperitoneal air
Jejunum
Perforation somewhat more likely than hematoma
Image Gallery
 Frontal radiograph obtained as part of a postmortem skeletal survey shows a midshaft left tibial fracture  in this 3 month old with numerous fractures and devastating intracranial injury. in this 3 month old with numerous fractures and devastating intracranial injury. |
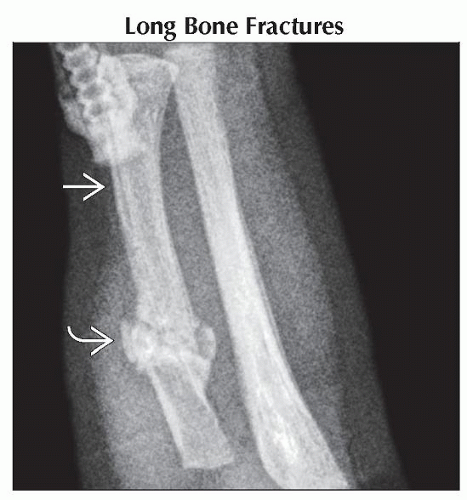 AP radiograph shows callus
 and periosteal reaction and periosteal reaction  around a radial fracture in a 2 month old with multiple fractures of varying ages and intracranial hemorrhage. around a radial fracture in a 2 month old with multiple fractures of varying ages and intracranial hemorrhage.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|