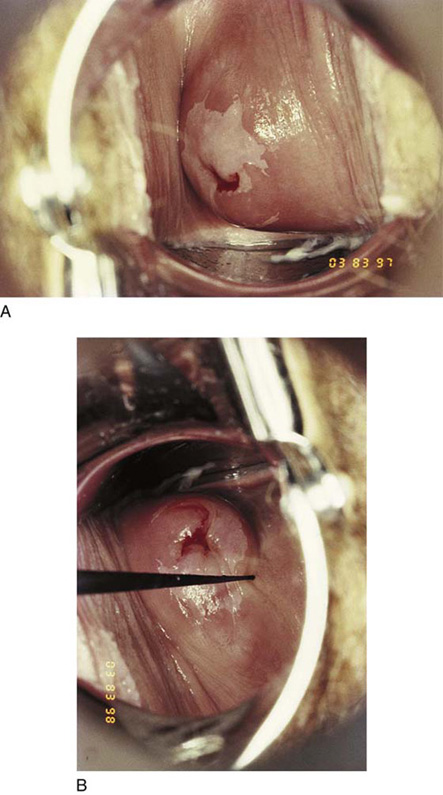
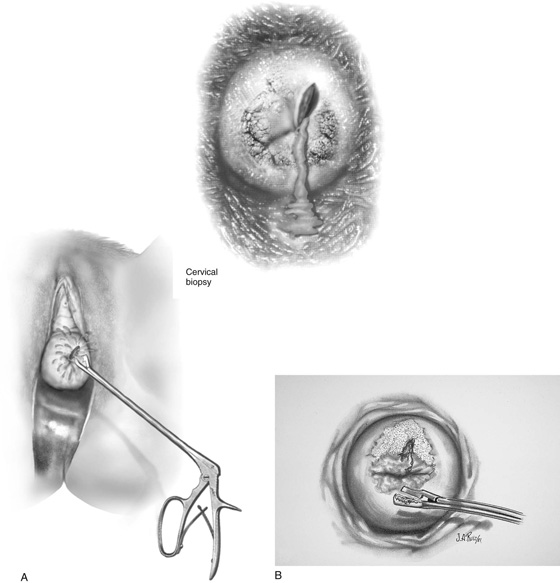
CHAPTER 45 All cervical biopsies should be colposcopically directed. There is no reasonable excuse for not performing a directed biopsy in the 21st century. The abnormal transformation zone is identified by applying acetic acid 3% to 4% to the cervix with a cotton swab and then observing the whitish color that develops in the atypical area with or without vascular abnormalities (Fig. 45–1A, B). The areas selected for biopsy are based on the severity observed colposcopically. Analgesia usually is not required if the biopsy is performed in a timely fashion and if the biopsy forceps are suitably sharp. For patients anxious about the biopsy, 1% lidocaine may be injected directly into the cervix using a 1½-inch 25- to 27-gauge needle. Most patients experience a pinching or light cramping sensation at the moment of biopsy. The biopsy forceps are manipulated to the operative site by utilizing the magnification of the colposcope to guide it to the appropriate location (Fig. 45–2A, B). The large teeth of the forceps stabilize the cervix so that its rounded surface will not slip away from the clamp (Fig. 45–3). The jaws are closed, and with a click a piece of tissue is cut away from the cervix and is held within the jaws of the biopsy clamp (Fig. 45–4). The specimen is handed off, and a cotton-tipped applicator soaked with Monsel’s solution (ferric subsulfate) is thrust into the crater at the biopsy site, held in place, and then slowly rolled to left and right until all bleeding stops (Fig. 45–5A, B). If bleeding does not stop following the application of Monsel’s solution, or if pulsatile bleeding is observed, a 3-0 Vicryl figure-of-8 suture should be placed while the magnification of the colposcope is used to accurately locate the stitch. A long, straight needle holder or a Haney needle holder should be used for this procedure (Fig. 45–6). Alternatively, a biopsy may be performed with a large loop electrode (Fig. 45–7A, B). FIGURE 45–1 A. Colpophotograph of the cervix shows an atypical transformation zone involving predominantly the anterior lip of the cervix but also the posterior lip. B. A titanium hook is utilized to determine the ectocervical extent of the lesion. FIGURE 45–2 A. A directed biopsy of the cervix is performed. The inset demonstrates schematically the colposcopic view obtained. B. An adequate sample will fill the cup of the biopsy forceps and will be sharply cut away from the surrounding cervical tissue.
Cervical Biopsy, Endocervical Curettage, and Cervical Biopsy During Pregnancy
Cervical Biopsy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


