FIGURE 8-1 Prenatal ultrasound depicting central deficiency of the hand.
CLINICAL QUESTIONS
- What are the genetic causes of cleft hands?
- What are the associated conditions, if any, with typical cleft hands?
- How are cleft hands classified?
- Is there nonoperative treatment?
- What are the surgical principles for typical cleft hands?
- What are the expected results of surgical treatment?
- What are the complications?
THE FUNDAMENTALS
Approach the game with no preset agendas and you’ll probably come away surprised at your overall efforts.
—Phil Jackson
Functional grasp, pinch, and release are critical for independent activities of daily living. Less than the full complement of independent, aligned, mobile fingers and thumbs can limit function. Bilateral disorders, even in the presence of a normal-functioning brain, can compromise opportunities and choices in life. So can unilateral hand disorders, though less so. Cleft hands are usually bilateral and always have digital absence and deformities. The cosmetic and social concerns and implications of cleft hands are real and important for the child and family.
Typical (ectrodactyly) (Figure 8-2) and atypical (sym-brachydactyly) (Figure 8-3) cleft hands are rare. With ectrodactyly, the basic principle is to close the cleft and deepen the first web space in order to preserve or enhance grasp, pinch, and release, as well as to improve cosmesis. This chapter mostly addresses typical cleft hands. Symbrachydactyly treatment is also covered in Chapter 9.

FIGURE 8-2 Radiograph of middle finger metacarpal present supporting index finger phalanges and a part of index MCP joint. Index is super digit.

FIGURE 8-3 Atypical cleft hand, symbrachydactyly. This is usually unilateral with negative family history.
Etiology and Epidemiology
Cleft hands occur in 1:10,000 to 1:90,000 live births depending on phenotypic classification.1,2 There is a clear genetic basis for typical cleft hands. Phenotypic expression is variable with approximately 70% of individuals with the genetic abnormality having clinical manifestations. Clefts can be present in one to four limbs. There is considerable variability in the degree of hand and foot abnormalities, but central deficiencies are always present.
The genetic basis for cleft hands is well founded in scientific research. Split hand–split foot malformations (SHFMs) are autosomal dominant disorders with variable penetrance. There are five distinct SHFM types with Dlx homeobox gene abnormalities. Ectrodactyly-ectodermal dysplasiascleft lip/palate (EEC) syndromes are due to p63 mutations, an ectoderm-specific transcription factor. The p63 and Dlx proteins colocalize in the nuclei of the apical ectodermal ridge (AER). There is increasing scientific evidence of a transcriptional cascade of events that contributes to ectodermal development with p63 mutations affecting Dlx homeobox gene regulation.3 A reduction in dactylin transcription is another contributing factor in some cleft hands.4,5
Cleft hands have been described as a longitudinal central deficiency (type IB International Federation of Societies for Surgery of the Hand [IFSSH] classification).6 Symbrachydactyly has been classified as an undergrowth (type V). More recently, the Japanese Society for Surgery of the Hand proposed a modification to the IFSSH classification7 with (1) all forms of symbrachydactyly being reclassified as type I (longitudinal [1B] or transverse [1A] deficiency) and (2) a new category of failure of ray induction to include typical cleft hand (previous type I), central polydactyly (previous type III), and bony syndactyly (previous type III). This is based on experimental work with embryonic rats treated with a chemotherapeutic agent (busulfan). In this animal model, cleft hands, central polydactylies, and osseous syndactylies were all created from defects in the central hand plate due to failure of induction.8 The experimental data indicate there is diffuse cell death in the central ectoderm and mesoderm with regression of fibroblast growth factor in the AER and bone morphogenetic protein-4 and sonic hedgehog in the mesoderm. A similar pattern of interdigital apoptosis and cartilage condensation leads to abnormal induction of digital rays in cleft hands, central polydactylies, and osseous syndactylies.9,10 There is one clear case of maternal chemotherapy for breast cancer in the first trimester resulting in cleft hands.11
Clinical Evaluation
There is never trouble diagnosing a cleft hand at birth. In fact, many are now diagnosed by prenatal ultrasound. The basic anatomy of four longitudinally aligned metacarpals, supporting four sets of longitudinally aligned, independent triphalangeal digits, with stable, mobile joints, is not present in centrally deficient hands. In addition, the thumb ray is rarely normal. So, evaluation begins by examining every anatomic structure of the hand and determining what is present or absent, what is normal or abnormal. This includes detailed soft tissue specifics, which can be overlooked (such as metacarpophalangeal joint [MCP] ligament stability in the index finger). These hands are so different that you truly need to start at the beginning and move precisely and methodically through clinical and radiographic exam features, ending ultimately with an intraoperative assessment of the anatomy. The surgeon can feel like an airplane pilot doing his or her exacting preflight checks: “Mobile thumb present … Check … Middle finger metacarpal present … No … Small finger normal size … No …” and so on. A high level of detail matters. Surgeons often focus only on the bony structures, which limits the precise understanding and treatment of these unique hands.
Clefts can be central, radial, less commonly ulnar, or in various combinations.12,13 The central cleft is usually V shaped with absent middle finger phalanges. In the mildest clefts, the middle finger phalanges are merely hypoplastic. The middle finger metacarpal can be absent, hypoplastic, bifid, or duplicated. The degree of involvement of the cleft may extend beyond the absence of the middle ray to include adjacent index and ring finger rays. The ultimate cleft is the presence of the small finger only, adhering to Maisels’ digital suppression sequence.14
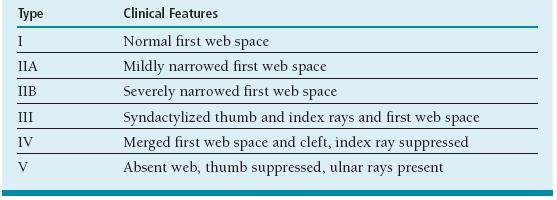
There are general clinical and radiographic patterns used to classify cleft hands. Nutt and Flatt used the number of digits absent (one, two, or three) as the basis of their classification. Ogino used a similar method but has five subtypes. There are also unusual subsets such as hands with six metacarpals15 or with transverse bones across the cleft.16 Manske and Halikis based their classification of the more common central and radial deficiencies on the status of the first web space (Table 8-1). The spectrum of first web-space changes extends from a normal (I), to narrowed (IIA mild, IIB severe), to syndactylized (III), to merged (IV absence of both index and long finger rays), to an absent first web space (V absent thumb, only ulnar ray[s]). This classification helps surgical planning as closure of the cleft requires a functional thumb and adequate first web space to obtain equivalent or better grasp and pinch function.
Table 8.1
Manske and Halikis based their classification of central deficiency on the status of the first web space17
Clefts may be unilateral, bilateral, or include one or both feet. The more deficient the first web space (types IIIB–V), the more likely there is to be bilateral hand and foot involvement (23% in Nutt, Flatt study).18 Often there is fourth web-space syndactyly and hypoplasia of the small finger. Clinodactyly, bracketed epiphyses, joint malalignment, and instability are common. Bilateral hand and foot clefts are the most common presentation in SHFM; ulnar clefts are rarer. The ring finger ray may be hypoplastic, partially or completely absent. With complete absence of the small finger or small and ring finger rays, it may be hard to determine if the clinical presentation is a part of mild ulnar dysplasia or an ulnar cleft hand.
Increased incidence of congenital heart disease has been observed in SHFM 1 and SHFM 5 genetic variations.19 EEC by definition has ectodermal dysplasia, cleft lip/cleft palate, and dental anomalies. In addition, EEC has an increased incidence of genitourinary abnormalities.20 Patients with cleft hands and feet have also been shown to have an increased incidence of encephalocele.21 Cleft hands have been described in Cornelia de Lange syndrome.22 There have been rare reports of associated deafness.
Surgical Indications
If you’ve got nothing to do, don’t do it here.
—Brenden “Buff” Blackler
Simple clefts are highly functional;23 more severe clefts have greater functional impairment. Since the brain is normal in these individuals, adaptive function can be high even in the presence of bilateral, marked anatomic variations. Surgery therefore needs to maintain or improve hand function over what is expected from natural history.
Surgical excision of a transverse bone in the cleft with progressive deformity is clearly indicated.16
The psychosocial stigmata of the cleft can vary by individual, family, ethnic group, geographic location, and generations (Figure 8-4). There is no doubt that these children and adults appear differently than noninvolved peers. How they feel about it and whether you can change that by surgery is unclear. However, most cleft operations are indicated to decrease deformity by cleft closure while maintaining or improving hand function by thumb and first web-space reconstruction.
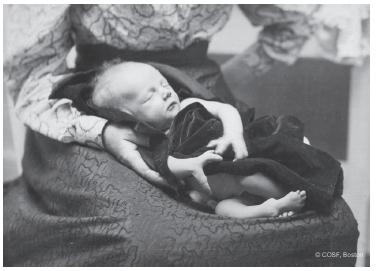
FIGURE 8-4 Children’s Hospital Boston archive photograph from late 1880s reveals the appearance of the SHFM has not changed in more than a century.
SURGICAL PROCEDURES
My players understand that preindenttion is most important.
—Ben Jacobson, after Northern Iowa upset over number one seed Kansas in the 2010 NCAA men’s basketball tournament
The principle of surgery for cleft hands is simple: close the cleft and optimize the first web-space and thumb function. This applies to Manske and Halikis types I to IV It is more complicated in the complex deformities with malaligned, unstable, and/or stiff digits adjacent to the cleft. The best outcomes are in the best hands with the best thumbs. Makes sense, right? Even with the busy, referral- and tertiary-care–based practice, cleft hand surgery is rare. Even a high-referral pediatric hand surgeon will maximally see only about two patients and do up to four operations a year if there is bilateral involvement.19 Tonkin and Wood, two senior, very practiced pediatric hand surgeons, presented jointly on their results of 12 Snow-Littler procedures. Experience is hard to come by and counts in these operations.
There is limited to no role for novice or intermediate-skill level surgeons in cleft hands except for (1) the simplest of clefts with near normal thumbs, (2) the gifted surgeon (by definition an immediate, expert surgeon), or (3) problems of patient access to expert surgeons. In any of those circumstances, we recommend case consultation before proceeding. With cleft hands, you need to work your way up to the black diamond level by gaining surgical expertise with other conditions and then applying prior experience to cleft surgery
 Simple Z-Plasty Deepening of First Web Space, Barsky Closure of Cleft
Simple Z-Plasty Deepening of First Web Space, Barsky Closure of Cleft
Nobody’s a natural. You work hard to get good and then work to get better.
—William James
The cleft closure in types I and IIA thumbs requires creation of a web commissure between the index and ring fingers. The Barsky flap (see Sidebar) is very useful in these circumstances (Figure 8-5). Similarly, simple, separate Z-plasty flaps (see Sidebar, Chapter 2) can be utilized to deepen the first web space and improve thumb function. Bilateral surgery can be done at the same setting in these relatively uncomplicated situations depending on the patient’s age, family wishes, and surgeon’s preference.
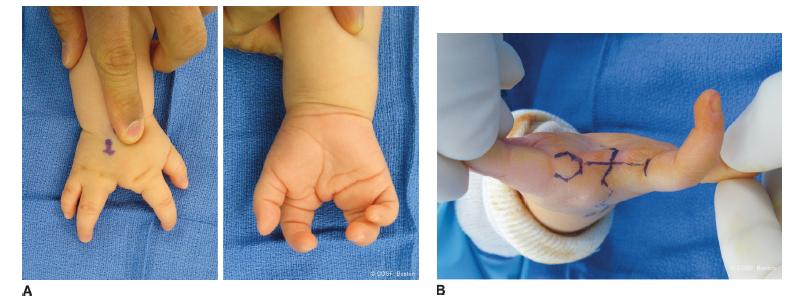
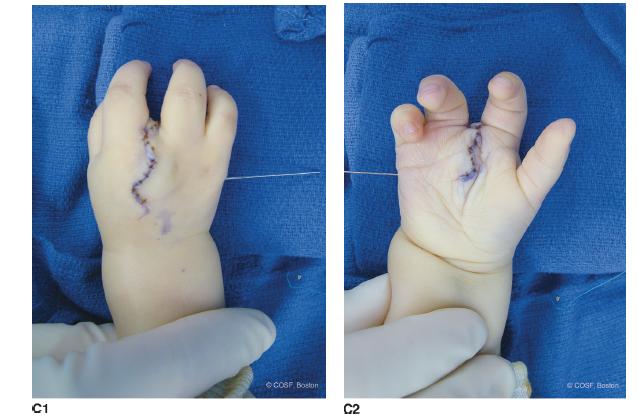
FIGURE 8-5 A: Typical cleft hand as a part of SHFM with dorsal and palmer views. B: Barsky flap outline for cleft closure in the same patient. C1: Dorsal view of cleft closure after intermetacarpal ligament reconstruction by local tissue and periosteal repair. C2: Palmar view photograph after redundant skin excision, Z-plasty closure of volar skin, web reconstruction, and pin fixation for postoperative stability.
SIDEBAR
Barsky Flap
The distally based diamond or hexagon is outlined on the radial aspect of the ring finger in the midaxial line to dorsal aspect of the proximal phalanx. The level of the hexagon on the ring finger corresponds to the transverse portion of the T on the ulnar aspect of the index finger proximal phalanx. The flap is then at the desired level of the created web. The hexagon is broad based enough to prevent flap necrosis and have an adequate web. Elevation of the flap is done carefully from proximal to distal while protecting the underlying neurovascular bundle. The incision continues from the proximal square aspect of the hexagon across the rim of the cleft and up the ulnar aspect of the index finger. The incision ends in a T. The horizontal portion of the T is correspondingly set at the level of the planned web. The width of the T is broad enough to accept the square base of the hexagon. Similarly, dissection on the radial aspect of the proximal aspect of the index finger is performed while protecting the underlying neurovascular bundle. The ring finger hexagon insets into the index finger rectangular flaps without tension once the cleft is closed and transmetacarpal ligament reconstruction is completed. The palmar and dorsal flaps are repaired to the web flaps after excision of the redundant skin. All sutures are placed without tension and close to the edge to preserve vascularity to the random pattern flaps (Figure 8-5B).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


