Mechanisms of increased vascular permeability
Chemical mediators Broadly speaking, the chemical mediators of inflammation originate either from plasma or from cells (Table 23.3). The production of active chemical mediators is triggered by microbial products or by products of the complement, kinin and coagulation systems. The mediators are generally short‐lived and removed by phagocytes. This system of balances and checks generally results in avoidance of the possible excess damage by these chemicals.
| Chemical mediator | Source |
|---|---|
| Histamine | Mast cells, platelets |
| Serotonin | Platelets, mast cells |
| Prostaglandins | Leucocytes, platelets, endothelium |
| Cytokines, nitric oxide | Macrophages, endothelium |
| Kinins | Plasma |
Chronic inflammation Acute inflammation may resolve completely, heal by fibrosis, result in abscess or progress to chronic inflammation (Figure 23.2). Although difficult to define precisely, chronic inflammation is considered to be inflammation of prolonged duration. Chronic inflammation can be a continuation of acute inflammation or start de novo. Chronic inflammation is characterised by concurrent tissue destruction and inflammation. The tissue changes include mononuclear cell infiltration, small vessel proliferation and fibrosis.
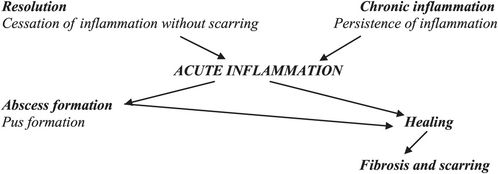
Outcomes of acute inflammation
Granulomatous inflammation Is a specific type of chronic inflammation characterised by the presence of granulomas in the diseased tissue. Granulomas are collections of macrophages referred to as epithelioid cells. When the granulomas show loss of cellular detail with cheese-like material centrally, it is termed caseating granulomas of which tuberculosis is the classical example. Giant cells (multinucleate cells) are seen and when they have nuclei arranged peripherally in a horseshoe shape they are termed Langhans type of giant cells. Sarcoidosis is the prototypical example of noncaseating granuloma. Sarcoid granulomas can occur anywhere in the body with lymph node, lung and skin being commoner sites. Kveim test, where granulomas are induced by injection of sterile sarcoid tissue homogenate is a positive response indicative of sarcoidosis. In nearly a third of patients with sarcoidosis, the serum level of angiotensin-converting enzyme is raised.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


