Background
Bupropion is used to treat depression during pregnancy. However, its usefulness as a smoking cessation aid for pregnant women is not fully known.
Objective
The objective of the study was to evaluate the preliminary efficacy of bupropion sustained release for smoking cessation during pregnancy.
Study Design
We conducted a randomized, prospective, double-blind, placebo-controlled, pilot trial. Pregnant women who smoked daily received individualized behavior counseling and were randomly assigned to a 12 week, twice-a-day treatment with 150 mg bupropion sustained release or placebo. The primary study objectives were to determine whether bupropion sustained release reduces nicotine withdrawal symptoms on the quit date and during the treatment period compared with placebo and whether it increases 7 day point prevalence abstinence at the end of the treatment period and at the end of pregnancy.
Results
Subjects in the bupropion (n = 30) and placebo (n = 35) groups were comparable in age, smoking history, number of daily smoked cigarettes, and nicotine dependence. After controlling for maternal age and race, bupropion sustained release reduced cigarette cravings (1.5 ± 1.1 vs 2.1 ± 1.2, P = .02) and total nicotine withdrawal symptoms (3.8 ± 4.3 vs 5.4 ± 5.1, P = .028) during the treatment period. Administration of bupropion sustained release reduced tobacco exposure, as determined by levels of carbon monoxide in exhaled air (7.4 ± 6.4 vs 9.1 ± 5.8, P = .053) and concentrations of cotinine in urine (348 ± 384 ng/mL vs 831 ± 727 ng/mL, P = .007) and increased overall abstinence rates during treatment (19% vs 2%, P = .003). However, there was no significant difference in 7 day point prevalence abstinence rates between the 2 groups at the end of medication treatment (17% vs 3%, P = .087) and at the end of pregnancy (10% vs 3%, P = .328).
Conclusion
Individual smoking cessation counseling along with the twice-daily use of 150 mg bupropion sustained release increased smoking cessation rates and reduced cravings and total nicotine withdrawal symptoms during the treatment period. However, there was no significant difference in abstinence rates between groups at the end of medication treatment and at the end of pregnancy, likely because of the small sample size. A larger study is needed to confirm these findings and to examine the potential benefit/ risk ratio of bupropion sustained release for smoking cessation during pregnancy.
Despite the well-known obstetrical, fetal, and developmental complications associated with cigarette smoking, 15.9% of all pregnant women continue to smoke throughout pregnancy. Behavioral interventions are only modestly effective in helping pregnant women quit smoking. Smoking-cessation medications increase the chance of quitting smoking in men and nonpregnant women, and they could also be used to reduce cigarette cravings and withdrawal and to enhance quit rates during pregnancy.
Bupropion sustained release (SR), an antidepressant, is commonly used to promote smoking cessation in males and nonpregnant females. The effectiveness of bupropion (Zyban, Wellbutrin) as a smoking cessation aid for pregnant women was suggested in a prospective observational study, in which pregnant smokers receiving bupropion 150 or 300 mg daily had higher quit rates than controls.
Based on this information, we conducted a randomized, prospective, double-blind, placebo-controlled, pilot trial of the preliminary efficacy of bupropion SR in combination with behavioral counseling for smoking cessation during pregnancy. The primary study objectives were to determine the following: 1) whether bupropion SR reduces nicotine withdrawal symptoms on the quit date and during medication treatment and 2) whether bupropion SR increases 7 day point prevalence abstinence at the end of medication treatment and at the end of pregnancy compared with placebo. Secondary objectives included the assessment of bupropion SR on overall quit rates during treatment and on adverse effects during pregnancy when compared with placebo.
Materials and Methods
Prior to implementation, the study protocol was reviewed and approved by The University of Texas Medical Branch (UTMB) Institutional Review Board and was registered on Clinicaltrials.gov ( ClinicalTrials.gov , identifier NCT01390246 ). An independent Data Safety and Monitoring Board reviewed ongoing trial data, including efficacy rates and serious adverse events (SAEs) through the study.
Recruitment
Pregnant smokers were recruited through the UTMB Department of Obstetrics and Gynecology clinics and the UTMB Regional Maternal Child Health Program clinics. Referrals from heath care providers were also accepted. In addition, the study was advertised through printed flyers, posters, and electronic media in Regional Maternal Child Health Program clinic waiting areas. Pregnant smokers who expressed interest in the research study were then screened for eligibility using inclusion and exclusion criteria.
Inclusion and exclusion criteria
Inclusion criteria were as follows: women ≥18 years of age between 13 and 30 weeks’ gestation, smoking ≥10 cigarettes per day (CPD) prior to pregnancy and 5 CPD for the preceding 7 days, English or Spanish speaking, and having the intent to carry to term.
Exclusion criteria were current illicit drug or alcohol abuse or dependence; multiple gestation; treatment for a psychiatric disorder within the last 6 months; unstable medical problems (pregnancy-induced hypertension [blood pressure (BP) >140/90 mg Hg], preeclampsia, threatened abortion, hyperemesis gravidarum); known fetal congenital abnormality; seizure disorder; use of psychotropic medication; use of medication known to lower the seizure threshold; anorexia/bulimia; a personal history of closed head trauma with >30 minutes of loss of consciousness or amnesia or resulting in a skull fracture or subdural hematoma/brain contusion; current use of any other smoking cessation treatment; and current use of methadone.
Consent and randomization
Prior to participation in the study, all subjects agreed and signed the institutional review board–approved informed consent. To ensure comparability of subjects in the treatment groups, we used the urn randomization method. The groups were balanced for 2 variables: gestational age at study entry and number of CPD. Subjects, primary investigators, and research nurses were blinded to pharmacotherapy group assignment.
Study design
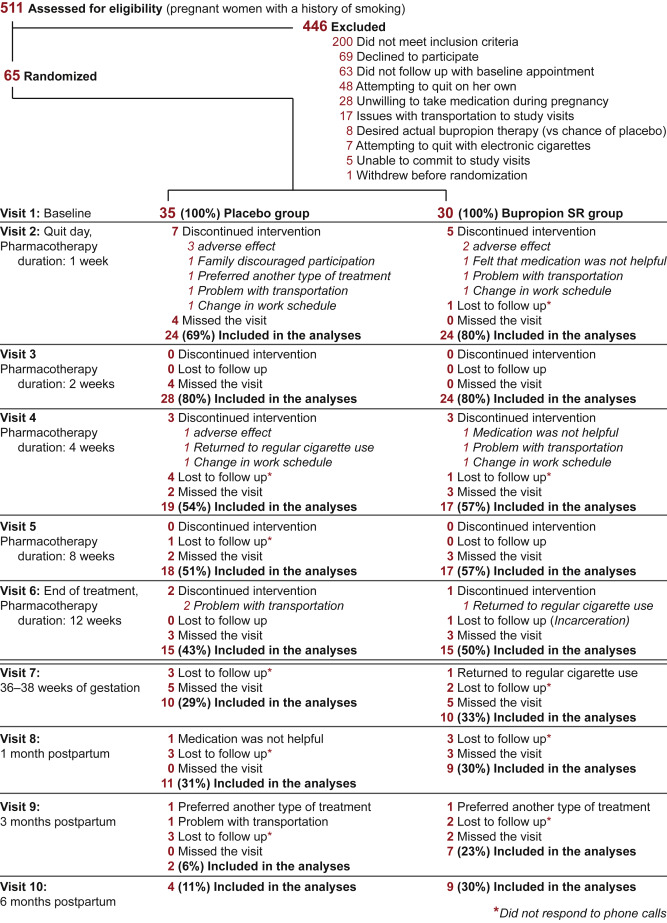
The study protocol consisted of 10 visits: first, enrollment, randomization, and study medication dispensation; second, the scheduled quit date; third to sixth, medication therapy progress assessment; seventh, the end of pregnancy (36–38 weeks’ gestation); and eighth to tenth, 1, 3, and 6 month postnatal assessments of abstinence ( Figure 1 ). Participants received either bupropion SR or matched placebo orally once daily for 3 days followed by twice daily for a total medication treatment of 12 weeks.
The University of Iowa Pharmaceuticals (Iowa City, IA) was contracted for production, labeling, and bottling of the active drug and placebo tablets. To confirm patients’ proper use of medication, participants were asked to keep a daily diary of the number of pills taken. Subjects then returned the study drug bottles at the next study visit to the research nurse who performed pill counts for compliance records. Compliance to study medication was also biochemically confirmed as described in the following text in the Biochemical measures section.
Both groups received behavioral interventions, which included 35 minute counseling sessions at each of the first 2 visits (enrollment and on the quit day) and 10 minutes of smoking cessation counseling at subsequent visits. Counseling sessions were delivered by a research nurse using a motivational interviewing approach, which was previously shown to be effective in pregnant smokers.
Measures
Prior to the smoking intervention, baseline standardized questionnaires assessed demographics, and smoking history/status as well as medical and obstetrical history. Additional questionnaires assessed the confidence and motivation to quit, concerns about excessive weight gain, and confidence in bupropion as a smoking cessation aid. The questionnaires were based on the clinical trials published previously, and each parameter was measured using a 5 point scale (1, least likely/mostly disagree, 5, highly likely/mostly agree). Nicotine dependence was assessed using the 6 item Fagerstrom Test of Nicotine Dependence. The Minnesota Nicotine Withdrawal Scale (MNWS) and the Primary Care Evaluation Score questionnaires were completed at every visit, including baseline.
At every visit, a research nurse monitored the smoking status of all subjects (ie, CPD, exhaled carbon monoxide [CO]) and adverse events (AEs). Exhaled CO was measured using a Vitalograph carbon monoxide monitor (Lenexa, KS) according to the manufacturer’s recommendations. A urine sample was collected at each visit and stored at –80°C.
AEs, including SAEs, were assessed on all subjects during interviews by the research nurse at each study visit. We monitored for maternal AEs that could be related to bupropion, such as seizures, BP >140/90 mm Hg, headache, insomnia, rhinitis, dry mouth, and anxiety. We defined a priori which AEs would be considered fetal and neonatal SAEs: intrauterine fetal demise, preterm delivery (<34 weeks), clinically suspected fetal growth restriction, congenital malformations, cardiovascular anomalies, low birthweight (<10%), Apgar scores <7 at 5 minutes, and neonatal length of hospital stay >3 days. Research nurses also abstracted data on pregnancy and neonatal outcomes from electronic medical records after delivery.
Biochemical measures
The accuracy of self-reported smoking abstinence during study visits was confirmed by an exhaled CO level of <4 parts per million (ppm) and by urinary cotinine level of <50 ng/mL. Cotinine in urine was quantified using the validated liquid chromatography–mass spectrometry (LC/MS) method ; sample extraction was based on the procedure described by Petersen et al. Patients’ compliance to the study medication was confirmed by concentrations of bupropion in urine and its metabolites (hydroxybupropion and threohydrobupropion) using the method reported previously.
Retention
Subjects received phone call reminders prior to each study visit. If a participant missed the appointment, the research staff called to reschedule. If research personnel were unable to reach a subject after multiple attempts, the reason for withdrawal was identified as lost to follow-up. These subjects were classified as smokers for the purpose of the analysis. Subjects were reimbursed as follows: $35 for each of the visits 1–7, $50 for each of the visits 8–9, and $75 for visit 10. The participants received the compensation at the end of study visits 3, 6, 7, 8, 9, and 10.
Data analysis
The original sample was based on detecting a difference in MNWS symptoms (ie, cigarette craving and total withdrawal scores) between the bupropion and placebo groups as a measure of potential efficacy. The study was powered for 3 outcomes: cigarette cravings, total MNWS withdrawal scores, and quit rates. A previous study of smoking cessation in pregnant women reported a standardized difference of d = 1.0 for cravings and d = 0.6 for total MNWS. In addition, a study of Hurt et al (1997) reported a 45% quit rate among male and nonpregnant female smokers treated with bupropion SR for cessation, whereas a 19% quit rate was observed among those receiving placebo.
The initial targeted enrollment of 50 women per group would yield a power of 0.85 with an alpha of 0.05 to detect differences in total MNWS scores, 0.99 power to detect differences in craving scores, and 0.80 power to detect differences in quit rates. However, 2 years after the trial had initiated, the sample size was reestimated because the original calculations were overpowered for some measures and the enrollment into the study was more difficult than expected. Thus, 30 subjects per group was still sufficiently powered (0.80) for the craving score; however, the total MNWS score was powered to 0.65 and the quit rate to 0.60.
Baseline characteristics between groups were compared using a 2 sample Student t test for continuous variables and a χ 2 (or a Fisher exact test) for categorical variables. Likewise, the Student t and χ 2 tests were used to test for differences between groups on birth outcomes. For continuous outcome variables measured at each visit (MNWS, most smoking outcomes), a linear mixed model with a random effect for subject and fixed effects for group, time point, and the interaction was run. For dichotomous outcomes measured at each visit (abstinence, AE), a general estimating equation with a binomial distribution and logit link function and effects for group, time point, and the interaction was evaluated.
Results
Five hundred eleven pregnant women were approached by research nurses to determine their study eligibility. Of these subjects, 200 (39%) did not meet inclusion criteria, 246 subjects (48%) were not enrolled for various reasons ( Figure 1 ), and 65 pregnant women (13%) were enrolled in the study. Of the recruited 65 subjects, 30 were randomized to the bupropion group and 35 to the placebo group.
Demographic and baseline characteristics
Table 1 presents demographic and baseline characteristics of study participants. The average gestational age at enrollment was 18.9 ± 4.5 weeks. Participants reported average smoking of 18 ± 8 CPD prior to pregnancy and 12 ± 8 CPD at enrollment. The distribution of demographic and baseline characteristics was similar in both groups except race/ethnicity (49% white/non-Hispanic in the placebo group vs 77% white/non-Hispanic in the bupropion group, P = .011) and age (27.5 ± 6.5 years vs 24.5 ± 5.6 years, P = .051).
| Characteristics | Placebo (n = 35) | Bupropion (n = 30) | P value |
|---|---|---|---|
| Demographics | |||
| Age, y, mean (SD) | 27.5 (6.52) | 24.5 (5.56) | .051 |
| Race/ethnicity, n, % | |||
| White/non-Hispanic | 17 (49) | 23 (77) | .011 |
| White/Hispanic | 5 (14) | 3 (10) | |
| White/none reported | 1 (3) | ||
| Black/non-Hispanic | 13 (37) | 2 (7) | |
| Black/Hispanic | 0 (0) | 1 (3) | |
| Marital status, n, % | |||
| Single | 27 (77) | 23 (77) | .946 |
| Married | 8 (23) | 7 (23) | |
| Educational status, n, % | |||
| High school graduate or less | 25 (71) | 20 (67) | .831 |
| Some college | 10 (29) | 10 (33) | |
| Employment status, n, % | |||
| Unemployed | 19 (54) | 16 (53) | .199 |
| Employed part or full time | 16 (46) | 14 (47) | |
| Income estimate per year, n, % | |||
| <$10,000 | 18 (51) | 14 (47) | .679 |
| $10,000–$30,000 | 11 (31) | 11 (37) | |
| $30,000–$100,000 | 5 (14) | 5 (17) | |
| Not reported | 1 (3) | ||
| Obstetrical | |||
| Gestational age at randomization, weeks, days, mean (SD) | 18.2 (1.2) | 18.5 (1.4) | .826 |
| Smoking history | |||
| Age when started smoking, y, mean (SD) | 15.7 (5.4) | 14.8 (2.8) | .414 |
| Number of cigarettes per day before pregnancy, mean (SD) | 16.1 (6.2) | 19.6 (10.1) | .092 |
| History of drug use, n, % | |||
| None | 24 (68) | 21 (70) | .901 |
| Marijuana | 9 (26) | 7 (23) | |
| Cocaine | 1 (3) | 1 (3) | |
| Street drugs | 1 (3) | 1 (3) | |
| Living with smoker, n, % | |||
| No | 12 (34) | 6 (20) | 0.228 |
| Yes | 23 (66) | 23 (77) | |
| Not reported | 1 (3) | ||
| Nicotine dependence | |||
| FTND score, mean (SD) | 4.6 (1.9) | 3.9 (1.7) | .147 |
| Psychosocial status | |||
| Total PRIME score, mean (SD) | 4.3 (4.4) | 3.6 (4.9) | .127 |
| Motivation and confidence to quit | |||
| Motivation to quit smoking at this time, mean (SD) | 4.3 (0.9) | 4.0 (0.7) | .182 |
| Confidence to quit smoking at this time, mean (SD) | 3.5 (1.1) | 3.6 (0.8) | .989 |
a Values are numbers of participants unless stated otherwise.
Fifty-seven percent of women enrolled had previously tried to quit smoking during their current pregnancy. The average total Fagerstrom Test of Nicotine Dependence and Primary Care Evaluation scores as well as the average scores for motivation and confidence to quit did not differ among study groups ( Table 1 ). The average level of worries about excessive weight gain caused by intervention was not very high (2.4 ± 1.6), and many participants believed that bupropion would be helpful (mean score 3.9 ± 0.8) to them for smoking cessation.
Smoking abstinence
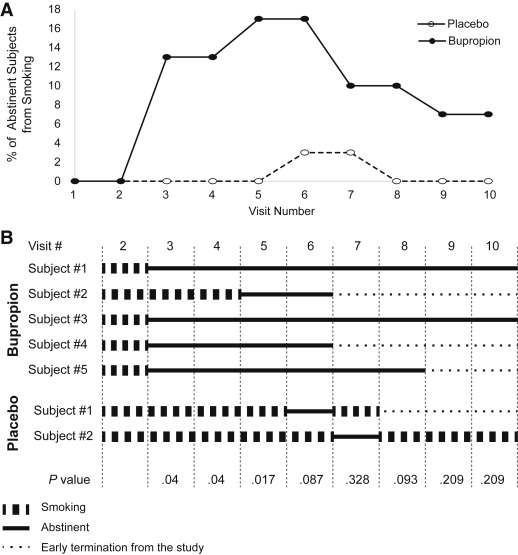
Seven day point prevalence abstinence was defined at each visit as no cigarettes (not even a puff) in the last 7 days, levels of CO in exhaled air <4 ppm, and concentrations of cotinine in urine <50 ng/mL. The point prevalence abstinence rates during the treatment assessment period (visits 2–6) between study groups were significant (2% in the placebo group vs 19% in the bupropion group, P = .003, Figure 2 ). There was no significant difference in abstinence rates between the bupropion and placebo groups at the end of medication treatment, visit 6 (17% vs 3%, P = .087), and at the end of pregnancy, visit 7 (10% vs 3%, P = .328), and during the postpartum period (visits 8–10).
Compared with baseline levels of self-reported cigarette consumption, there was at least a 50% reduction in cigarettes smoked per day during treatment, at the end of pregnancy, and postpartum in both groups ( Table 2 ). Although this reduction in cigarette consumption was not statistically significant between the groups, exhaled CO and urinary cotinine concentrations during treatment (visits 2–6) were higher in the placebo group than the bupropion group ( P = .011 and P < .001, respectively, Table 2 ).
| Variables | Placebo, mean (SD) | Bupropion, mean (SD) | P value | |
|---|---|---|---|---|
| Controlling for baseline | Controlling for baseline, age, and race | |||
| Cigarettes per day | ||||
| Baseline, visit 1 | 10.7 (6.9) | 13.4 (9.3) | .202 | |
| Quit date, visit 2 | 5.8 (4.3) | 7.2 (7.6) | .959 | .93 |
| Treatment assessment period, visits 2–6 | 5.0 (4.8) | 4.7 (6.3) | .068 | .216 |
| Weeks 36–38, visit 7 | 1.6 (2.5) | 4.6 (5.9) | .665 | .441 |
| Postpartum, visits 8–10 | 4.3 (3.9) | 4.1 (3.5) | .550 | .749 |
| Exhaled carbon monoxide, ppm | ||||
| Baseline, visit 1 | 10.2 (6.5) | 13.4 (8.5) | .117 | |
| Quit date, visit 2 | 8.7 (5.4) | 9.2 (7.3) | .509 | .988 |
| Treatment assessment period, visits 2–6 | 9.1 (5.8) | 7.4 (6.4) | .011 | .053 |
| Weeks 36–38, visit 7 | 5.5 (5.1) | 7.2 (4.7) | .514 | .662 |
| Postpartum, visits 8–10 | 8.6 (5.7) | 10.5 (8.6) | .613 | .745 |
| Cotinine, ng/mL | ||||
| Baseline, visit 1 | 822.7 (685.9) | 657.6 (479.4) | .295 | |
| Quit date, visit 2 | 843.5 (692.4) | 404.7 (402.9) | .066 | .240 |
| Treatment assessment period, visits 2–6 | 830.5 (727.3) | 347.8 (383.9) | < .001 | .007 |
| Weeks 36–38, visit 7 | 542.6 (671.2) | 484.1 (462.1) | .960 | .666 |
| Postpartum, visits 8–10 | 997.1 (609.8) | 755.5 (729.0) | .365 | .749 |
| Total score of withdrawal symptoms (no craving) | ||||
| Baseline, visit 1 | 4.43 (5.77) | 5.22 (6.05) | .620 | |
| Quit date, visit 2 | 4.88 (4.61) | 4.75 (4.87) | .978 | .713 |
| Treatment assessment period, visits 2–6 | 5.35 (5.14) | 3.77 (4.27) | .068 | .028 |
| Craving for tobacco | ||||
| Baseline, visit 1 | 1.79 (1.64) | 1.63 (1.55) | .742 | |
| Quit date, visit 2 | 2.33 (1.31) | 2.04 (1.08) | .786 | .622 |
| Treatment assessment period, visits 2–6 | 2.07 (1.23) | 1.50 (1.11) | .08 | .020 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


