Board Simulation: Potpourri
Elumalai Appachi
QUESTIONS
1. A 9-month-old infant presents with fever, irritability, and petechial rash for 1 week. He has had multiple ear infections in the past and has a draining right ear. He has seborrhea on his scalp and hepatosplenomegaly on abdominal examination. A radiograph of the skull is shown in Figure 67.1. Radiography of the chest shows multiple pulmonary infiltrates. Which of the following is a true statement regarding this infant’s condition?
a) A short course of methylprednisolone along with intravenous antibiotics is indicated.
b) A bone scan will be diagnostic.
c) The rash is always caused by thrombocytopenia.
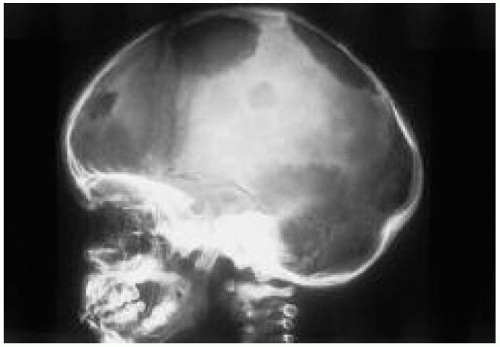 Figure 67.1 Skull radiograph of the patient in question 1. See explanation of question 1 for details. |
d) The serum sodium level may be elevated.
e) The prognosis is excellent with appropriate therapy.
View Answer
Answer
The answer is d. Langerhans cell histiocytosis is a multisystem disorder with a variable presentation. The skeleton is the most commonly affected site; osteolytic lesions are most often seen in the skull (Fig. 67.1). Chronically infected, draining ears are a frequent feature and associated with destruction of the mastoids. Skin involvement may be manifested as seborrheic dermatitis of the scalp or diaper area or as a petechial rash, even in the absence of thrombocytopenia. Localized or generalized lymphadenopathy with hepatosplenomegaly is also common. Infants with pulmonary disease and multiple infiltrates present with respiratory distress and progressive respiratory failure. Hypothalamic and pituitary dysfunction may result in growth retardation and diabetes insipidus, which may present as irritability, dehydration, and hypernatremia. Systemic manifestations include fever, weight loss, irritability, and failure to thrive. Skeletal survey, tissue biopsy, chest radiography, a determination of the serum sodium level and urine osmolality, and a detailed evaluation of all organ systems are necessary to establish the diagnosis and plan therapy. Multisystem involvement requires systemic chemotherapy. The prognosis in infants with multisystem disease is poor.
2. An 8-year-old girl presents with a history of fever, joint pain, and rash for 3 days (Fig. 67.2). On exami nation, she has swollen ankle and knee joints, and a pericardial rub is heard on auscultation. Which of the following is the most appropriate next step in the management of this girl?
a) Obtain a throat culture before administering antibiotics.
b) Administer intravenous immunoglobulin therapy.
c) Administer high-dose intravenous methylprednisolone.
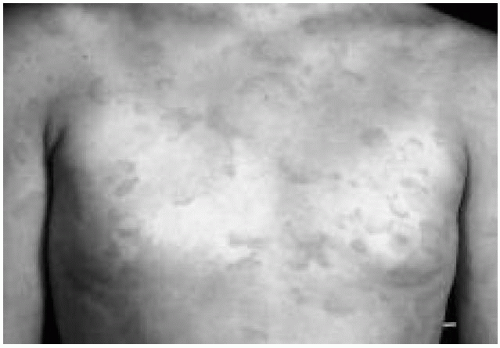 Figure 67.2 Rash in patient in question 2. See explanation of question 2 for details. (See color insert.) |
d) Perform knee joint aspiration at the bedside and send the aspirates for bacteriologic cultures.
e) Consult a cardiologist for pericardiocentesis.
View Answer
Answer
The answer is a. Acute rheumatic fever is difficult to diagnose, given that no single test or clinical sign confirms the diagnosis. The Jones criteria are helpful in making the diagnosis. The presence of erythema marginatum (Fig. 67.2), a lesion characterized by a serpiginous appearance and blanching in the middle, is one of the major criteria for the diagnosis of rheumatic fever. It often occurs in patients with carditis. The other major criteria include carditis, migratory polyarthritis, chorea, and subcutaneous nodules. The minor criteria include fever, arthralgia, elevated acute phase reactants (elevated sedimentation rate, increased C-reactive protein), and a prolonged PR interval on the electrocardiogram. The presence of two major criteria or of one major and two minor criteria with evidence of streptococcal infection strongly suggests rheumatic fever. However, when a child presents with unexplained chorea or carditis, the diagnosis of rheumatic fever should be considered, even if the criteria are not met. All patients with acute rheumatic fever should be treated for group A streptococcal infection. Immunoglobulin therapy is not indicated for the child in question. Corticosteroid therapy is indicated for patients with moderate to severe carditis. Pericardiocentesis is indicated if evidence of pericardial effusion and tamponade is present.
3. An 11-year-old boy presents with a history of fever, joint pain, and the rash pictured in Figure 67.3. He also has abdominal pain and a swollen scrotum. He had a streptococcal throat infection a week ago. Which of the following is a true statement regarding his condition?
a) He has poststreptococcal glomerulonephritis.
b) His platelet count is likely to be normal.
c) A lumbar puncture should be performed and the child should receive broad spectrum antibiotics.
 Figure 67.3 Rash in patient in question 3. See explanation of question 3 for details. (See color insert.) |
d) He has Kawasaki disease.
e) Bone marrow aspirate will be diagnostic.
View Answer
Answer
The answer is b. Henoch-Schönlein purpura is the most common cause of nonthrombocytopenic purpura in children. The etiology is unknown. Abdominal pain is usually secondary to vasculitis of the gastrointestinal tract and may mimic acute abdomen. Intussusception may occur occasionally. Scrotal edema and tenderness may mimic acute torsion of a testis. Renal involvement, in the form of hematuria, occurs in 25% to 50% of patients. Therapy with IV steroids is usually reserved for life-threatening intestinal and central nervous system complications. The diagnosis is based on the clinical features; routine laboratory tests are not necessary, and bone marrow aspiration is not indicated.
4. A 14-year-old adolescent girl (Fig. 67.4) presents with exertional dyspnea and palpitations. Examination reveals a heart murmur. Each of the following statements is appropriate regarding her diagnosis and management except:
a) She has a 25% chance of having an offspring with a similar condition.
b) She requires a slit-lamp examination of her eyes and an ophthalmologic evaluation.
c) She requires endocarditis prophylaxis for dental and invasive surgical procedures.
d) Therapy with propranolol is indicated in most cases.
e) A urinary cyanide nitroprusside test is indicated.
View Answer
Answer
The answer is a. Marfan syndrome is inherited in an autosomal-dominant pattern, but nearly 30% of cases are new mutations. Because the inheritance is autosomal-dominant, the chance that an offspring will be affected is 50%. Slit-lamp examination may reveal lens dislocation and iridodonesis. Morbidity is usually caused by cardiovascular defects, including aortic root dilatation, and mitral valve prolapse. Propranolol or atenolol may be used therapeutically to reduce cardiovascular morbidity. The cyanide nitroprusside test or specific amino acid assays can be performed to differentiate Marfan syndrome from homocystinuria.
 Figure 67.4 Hands of patient in question 4. See explanation of question 4 for details. |
5. A 13-month-old infant is brought to the emergency department with a 5-day history of high fever, bilateral non purulent conjunctivitis, fissured lips, maculopapular rash, joint swelling, and irritability. She received her measles-mumps-rubella vaccine 4 days ago. The next most appropriate step is to:
a) Reassure the parents that her symptoms are a reaction to the vaccine.
b) Administer intravenous penicillin and obtain an urgent electrocardiogram.
c) Administer high-dose intravenous methylprednisolone therapy.
d) Admit her and perform a lumbar puncture to rule out meningitis.
e) Consult a pediatric cardiologist for echocardiography.
View Answer
Answer
The answer is e. Kawasaki disease is an acute febrile vasculitis. Coronary artery dilatation and aneurysms are the most feared complications of this syndrome and occur in approximately 20% of untreated individuals. The diagnosis of Kawasaki disease is made clinically on the basis of diagnostic criteria. Adverse reactions to measlesmumpsrubella vaccine in the form of fever and rash classically develop 10 to 14 days after vaccination. Currently, corticosteroid therapy is not given initially to patients with suspected Kawasaki syndrome. Given the clinical picture, the next logical step is to obtain an echocardiogram to examine the coronary arteries and myocardial function. Depending on the child’s appearance, a lumbar puncture may be appropriate. Children
with Kawasaki syndrome can be so irritable that meningitis cannot be ruled out with confidence. In this instance, a lumbar puncture and empiric antimicrobial therapy are certainly warranted.
with Kawasaki syndrome can be so irritable that meningitis cannot be ruled out with confidence. In this instance, a lumbar puncture and empiric antimicrobial therapy are certainly warranted.
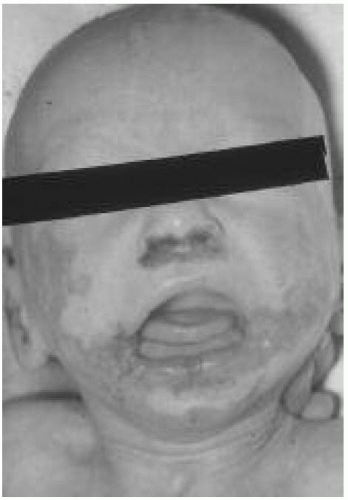 Figure 67.5 Eczematous lesions of patient in question 6. See explanation of question 6 for details. |
6. A 12-month-old infant is admitted for chronic enteritis, failure to thrive, and eczematous lesions over the perioral and perianal areas (Fig. 67.5). Which of the following is true regarding her condition?
a) Treatment with high-dose zinc and close monitoring of levels is indicated.
b) She may have an elevated serum alkalinephosphatase level.
c) Therapy with acyclovir is indicated.
d) A gluten free diet should be introduced slowly.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


