Ascariasis
John S. Schieffelin and Richard A. Oberhelman
 EPIDEMIOLOGY
EPIDEMIOLOGY
Ascariasis is caused by the intestinal roundworm Ascaris lumbricoides. The World Health Organization has estimated that more than 800 million people are infected with A lumbricoides, with the largest number of infections occurring in Asia.1,2 In areas of high prevalence, infection rates as high as 95% have been noted. Tropical areas with warm, wet climates favor year-round transmission and are more likely to have high prevalence rates. In the United States, the highest infection rates are among immigrants from developing countries (20–60% infected in some surveys). Young children are infected most frequently, with peak prevalence in children between the ages of 3 and 8 years living in the tropics. Intensity of infection or worm burden typically decreases significantly after the age of 15 years. Infections tend to cluster in families. Individuals may be asymptomatic and shed eggs for years, thus enhancing transmission.
 PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Ascaris is the largest intestinal roundworm that commonly infects humans: females measure 20 to 40 cm long, and males measure 15 to 30 cm long (eFig. 324.1  ).3 The female lays approximately 200,000 eggs daily; eggs are broadly ovoid and 45 to 75 μm by 35 to 50 μm. Fertilized eggs have a 3-layer coat with a bile-stained, mamillated outer shell. Unfertilized eggs are broader and longer (ie, approximately 90 μm by 45 μm) and usually lack the mamillated outer coat (Fig. 324-1).
).3 The female lays approximately 200,000 eggs daily; eggs are broadly ovoid and 45 to 75 μm by 35 to 50 μm. Fertilized eggs have a 3-layer coat with a bile-stained, mamillated outer shell. Unfertilized eggs are broader and longer (ie, approximately 90 μm by 45 μm) and usually lack the mamillated outer coat (Fig. 324-1).
Eggs are passed in the host’s feces and become infective in the environment only after the first-stage larva molts within the egg (embryonation). The eggs are resistant to drying, low temperatures, and many chemicals. Children often infect themselves and others by playing in the same areas where they eliminate their wastes. Where human wastes are used as fertilizer (eg, Asia), Ascaris infection is especially frequent.
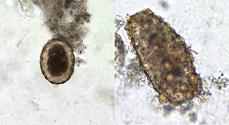
FIGURE 324-1. Fertilized (left) and unfertilized (right) Ascaris egg, 2000× magnification. (Source: http://www.dpd.cdc.gov/dpdx/HTML/Ascariasis.htm. Accessed January 13, 2008.)
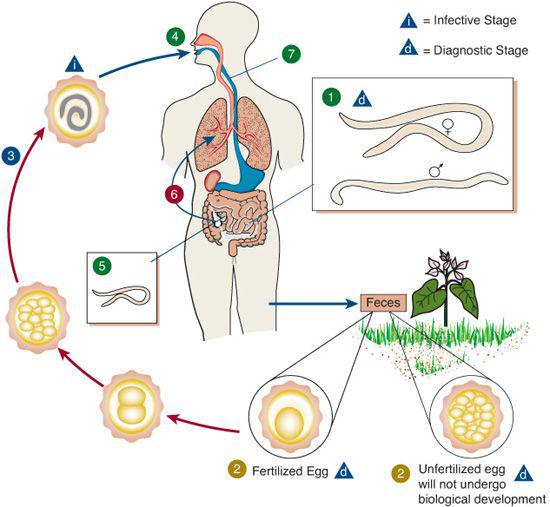
When embryonated eggs are ingested and stimulated by enzymes in the duodenum, the larvae emerge, traverse the intestinal mucosa, and enter the mesenteric lymphatics and venules (Fig. 324-2). They then enter the portal circulation and reach the pulmonary vascular bed, perforate the alveolar wall, ascend the respiratory tree to the epiglottis, and are swallowed. The vast majority of ascarids finally settle in the jejunum, where mature worms mate and females begin laying eggs in 2 to 2.5 months. After a life span of 10 months to 2 years, they are passed in the stool. A video showing a live worm observed during colonoscopy is available at: www.youtube.com/watch?v=HOaZCkA8Zvk (accessed December 4, 2009).
 CLINICAL MANIFESTATIONS
CLINICAL MANIFESTATIONS
During the period of larval invasion and migration, cough, dyspnea, fever (39.5°C/103.1°F) to 40.5°C/104.9°F), rales, and dullness to percussion of the chest may be evident. Invasion of the respiratory system by migrating larvae results in alveolar hemorrhages, and pulmonary damage may be extensive, especially with large numbers of larvae. Hemoptysis may occur, and larvae may be found in the sputum. Shifting, consolidated infiltrates, and widening of the pulmonary hilum may be seen, and the eosinophil count often is very high (Löffler syndrome). During this phase, other manifestations of hypersensitivity such as urticaria and wheezing may occur with repeated infections. Larvae occasionally may traverse the pulmonary circulation and produce serious lesions in the eye, central nervous system, and kidney, resembling visceral larva migrans caused by Toxocara larvae.
Unless they are numerous, adult worms in the small intestine generally are associated with few symptoms. The most frequently noted symptoms in children are vague epigastric pains, nausea, vomiting, and anorexia. Severe, intermittent, colicky abdominal pain at times may result from partial intestinal obstruction. The more serious problems encountered with Ascaris infection result from migration of adult worms into the bile and pancreatic ducts, where they may induce biliary stone formation, pancreatitis, small intestinal perforation, and complete intestinal obstruction with intussusception. Worms occasionally may migrate cephalad and emerge through the mouth or nose, or migrate posteriorly and pass through the rectum.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


