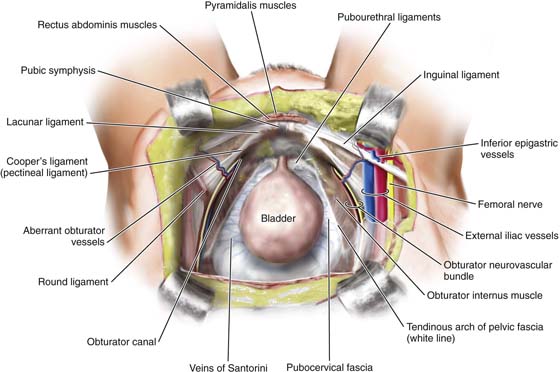
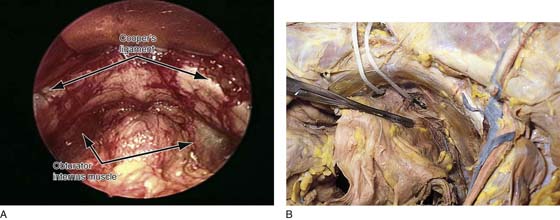
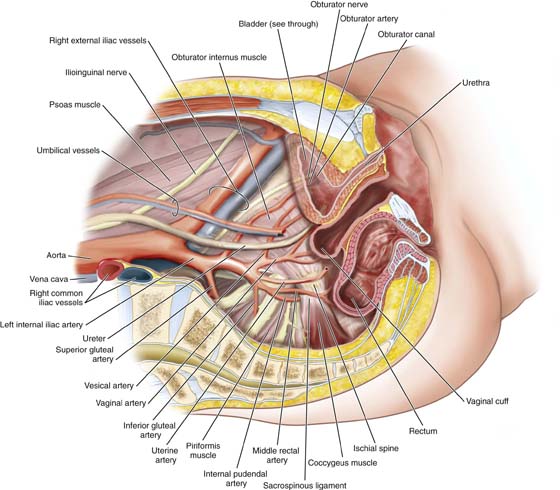
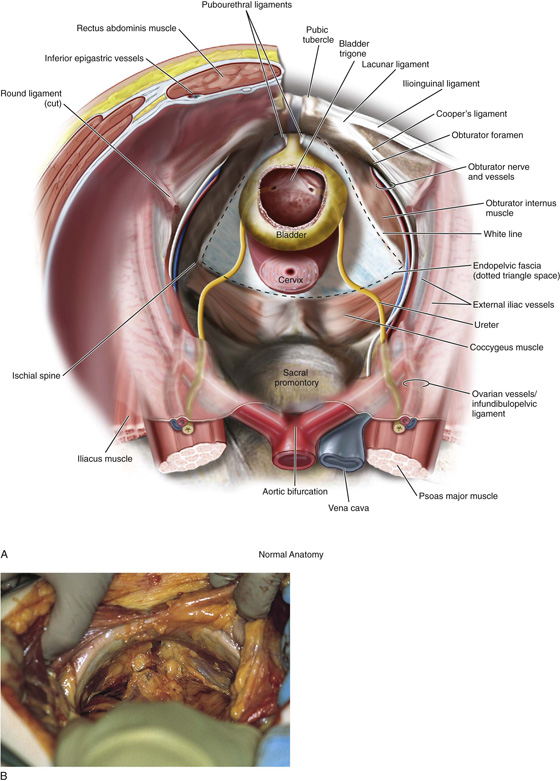
CHAPTER 31 Michael S. Baggish The boundaries of the retropubic space (space of Retzius) are the symphysis pubis anteriorly, the pubic rami laterally, and the sidewalls composed of pubic bone and obturator internus muscle. The anterior aspects of the proximal urethra and extraperitoneal portions of the bladder are seen upon exposure of the retropubic space. Figure 31–1 illustrates the view from above the retropubic space. Note that the floor of the retropubic space is formed by the fibrofatty outer lining of the vaginal wall termed endopelvic fascia, the perivesical fascia, and fibers from the levator ani muscle. This trapezoid structure provides support for the proximal urethra and bladder. Figure 31–2 shows a sagittal section of the normal anatomy of the pelvis. Figures 31–3, 31–4, and 31–5 demonstrate the relationship of the space to the urinary bladder, pelvic sidewall, upper thigh, and uterus. FIGURE 31–1 Normal anatomy of the pelvis viewed from above. Note how the proximal urethra and extrapertioneal portions of the bladder are exposed through the retropubic space. Note the trapezoid-shaped endopelvic fascia or inside lining of the muscular portion of the vaginal wall. The fascia provides the support for the anterior wall. FIGURE 31–2 Sagittal section of the normal anatomy of the pelvis. Note how the various vessels, nerves, and muscles relate to the bladder and retropubic space. Note now the external iliac vessels exit the pelvis underneath the inguinal ligament just lateral to the uppermost portion of the retropubic space, while the obturator neurovascular bundle passes through the retropubic space to exit the pelvis through the obturator canal. FIGURE 31–3 A. Surgical anatomy of the retropubic space. Note that the proximal urethra and bladder rest on the anterior vaginal wall with its underlying muscular component, or pubocervical fascia. The vagina attaches laterally to the white line, or arcus tendineus fasciae pelvis. The veins of Santorini run within the vaginal wall and are commonly encountered during colposuspension procedures. Other important vascular structures that may be encountered in this space include the obturator neurovascular bundle, the aberrant obturator artery and vein, and the external iliac artery and vein. B. Retropubic space in a female cadaver. Note that abundant retropubic fat is usually encountered upon initial dissection into the space. FIGURE 31–4 The uterus (U) is elevated via a fundal (blue) suture. The bladder (B) is held straight upward via a white stitch. The sawed pubic symphysis (P) is most forward (anterior). The mons veneris (M) has been cut and flapped forward anteriorly. FIGURE 31–5 A. Retropubic space in a live patient. The arrows point to the top lateral portions of the space noting Cooper’s ligament. Below this, the obturator internus muscle is seen on each side. Note again the abundant retropubic fat commonly seen in this space. B. The retropubic space has been totally exposed. A large straight clamp is placed across the urinary bladder. An umbilical tape has been placed just above the urethrovesical junction. The tip of a probe placed in the vagina protrudes through the internal projection of the right anterolateral fornix. The adipose tissue behind the symphysis between the bladder and the pubic bones can be gently separated by blunt finger dissection. The space is progressively developed from the superior to the inferior margin of the pubic symphysis (see Figs. 31–4, 31–5, and 31–6). The lateral development of the retropubic space extends to the perivesical space and terminates at the pelvic sidewall or, more precisely, at the obturator internus muscle (Fig. 31–7A–C and 31–8A, B). The lateral aspects of the retropubic space are demarcated in the dissections shown in Fig. 31–9A–F. The arcus tendineus originates from the obturator internus fascia. This whitish thickening of the obturator fascia can vary in its configuration from a single line to a wishbone or double-line structure. The pubococcygeus muscle (levator ani) in turn takes its origin from the arcus tendineus. The broad levator ani funnels downward into the depths of the pelvis. A portion of the levator ani arises from the inferior margin of the pubic ramus on either side in close proximity to the urethra, where it plays a key role in the sphincter mechanism to maintain urinary continence (see Fig. 31–8A, B). At the inferior extent of the space are located the urethrovesical junction, the anterolateral vaginal fornices, and the levator ani muscles (see Figs. 31–8A, B; 31–9A, and 31–10). The urethrovesical junction and the greater mass of the urinary bladder are exposed within the space of Retzius. Specifically, these structures lie on the floor of the retropubic space (Figs. 31–11A, B and 31–12). At the level of the proximal urethra, the pubourethral (puboprostatic) ligaments are noted; these are stylized in Figure 31–3. The actual structures run from the posterior symphysis pubis to the pubocervical fascia (endopelvic fascia) in contact with the proximal urethra on each side and are thought to be key structures for the maintenance of continence (Figs. 31–13A–D). The arcus tendineus fasciae pelvis, or white line, stretches from the posterior aspect of the symphysis pubis and continues in a downward sloping direction along the fascial margin of the obturator internus muscle to terminate at the ischial spine. The attachment of the pubocervical fascia (endopelvic fascia) to the white line partially maintains the support of the lateral vaginal wall. Detachments of the pubocervical fascia from the white line will lead to paravaginal defects. The arcus tendineus can be seen clearly (see Fig. 31–9A–F). It is a fascial landmark (see Figs. 31–11 and 31–12). From the point where the levator ani takes origin from the arcus, the muscle swings downward toward the midline, thus composing a portion of the pelvic floor (see Fig. 31–8B
Anatomy of Retropubic Space
 Mickey M. Karram
Mickey M. Karram
![]()
Stay updated, free articles. Join our Telegram channel


Full access? Get Clinical Tree


