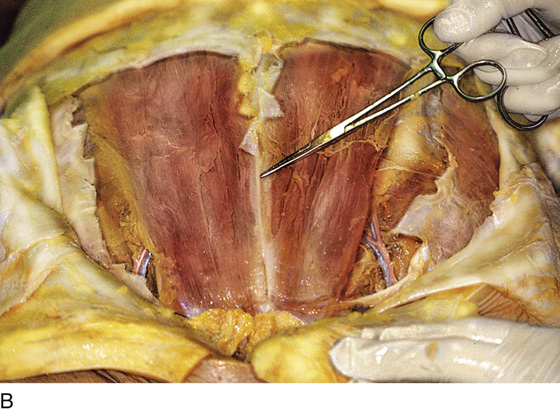
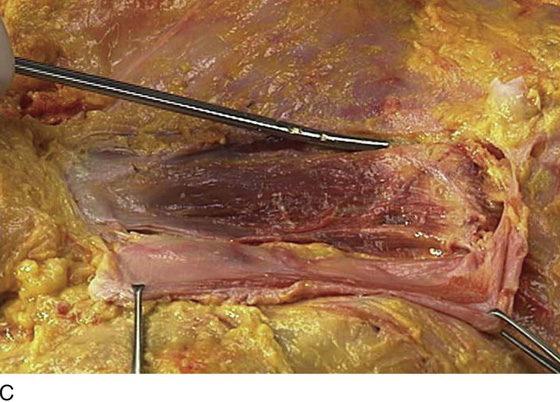
CHAPTER 7 The pelvic surgeon is mainly involved with the abdomen below or at the level of the umbilicus. The abdominal wall below the level of the umbilicus consists of skin, fat, fascia, and several relatively thin muscles. Specific skin and bony landmarks should be noted (e.g., the umbilicus roughly overlies the bifurcation of the aorta) (Fig. 7–1). The anterior superior iliac spine marks the origin of the inguinal ligament and of the sartorius muscle. The upper surfaces of the pubic bone and symphysis mark the terminus of the inguinal ligament and the insertion of the rectus abdominis muscle (Fig. 7–2). The cadaver is typically in the supine position (see Fig. 7–1). The abdominal wall from superficial to deep consists of skin, subcutaneous fat, fascia, muscle, properitoneal fat, and peritoneum. Once the skin and fat are dissected away, the gray-white glistening fascia comes into view (see Fig. 7–2). This is the superficial investment layer of the underlying muscle (Fig. 7–3). When all layers have been traversed, the peritoneal cavity is entered. The peritoneum of the anterior wall is called the parietal peritoneum, and the peritoneum investing the viscera is known as the visceral peritoneum. The large and small intestines are directly beneath the parietal peritoneum of the anterior abdominal wall (Fig. 7–4). The strength of the otherwise thin layer of muscle and fascia derives from the crisscrossing of various muscle fibers. The external oblique muscles are vectored downward (caudally) and medially. The rectus muscles run straight up and down (vertically) from the xiphoid to the symphysis pubis (Figs. 7–5 and 7–6). It is interesting to note that the tough fascial sheath of the rectus muscles is formed by contributions of other muscles of the anterior abdominal wall (i.e., the external oblique, internal oblique, and transversus abdominis muscles [Fig. 7–7]). At the point where the two rectus muscles join in the midline, a white line, aptly called the linea alba, is visible (see Fig. 7–5B). The fibers of the internal oblique muscle cross those of the external oblique. Similarly, the transversus abdominis muscle crosses both the internal and external oblique muscles as it vectors in an almost horizontal direction. Throughout, the posterior rectus sheath contains transversalis fascia (Fig. 7–8). The inguinal ligament and canal are seen in the lowest portion of the abdomen. Actually, the ligament is an anatomic boundary between the abdomen and the thigh (Figs. 7–9A–C and 7–10). As the external iliac vessels cross between the pubic ramus and the inguinal ligament, they become the femoral artery and vein. The inguinal ligament and the sartorius muscle of the thigh originate at the anterior superior iliac spine (Fig. 7–11A). The length of the inguinal ligament may be accurately estimated by placing one finger on the iliac spine and another finger on the pubic tubercle (Fig. 7–11B) and measuring the distance between these fingers. The internal inguinal ring is the point of entry (into the inguinal canal) for intra-abdominal structures, such as the round ligament. They exit the canal onto the abdominal wall via the superficial inguinal ring (Fig. 7–12A–E). FIGURE 7–1 Important skin surface landmarks include the umbilicus, the anterior superior iliac spines, the pubic symphysis, and the xiphoid process. FIGURE 7–2 After the lower abdominal flaps have been retracted, the gray-white fascia (aponeurosis) of the external oblique and rectus abdominis muscles is in clear view. The arrows indicate surface landmarks (umbilicus [upper arrow], anterior superior iliac spine [lower arrow], and upper margin of the pubic symphysis). FIGURE 7–3 Skin and fat have been retracted except for the area of the mons. The fascia of the external oblique and rectus abdominis is intact. FIGURE 7–4 The peritoneal cavity has been entered. The small and large intestines occupy the entire space within the lower abdomen. They constitute the most superficial viscus encountered in the abdominal cavity.
Anatomy of the Lower Abdominal Wall





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


