Allergic and Eosinophilic Gastroenteropathies
B U.K. Li
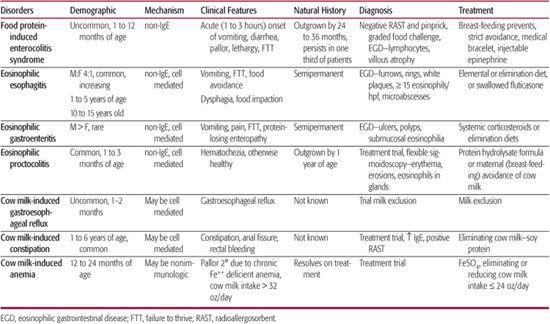
Allergic and eosinophilic disorders of the gastrointestinal (GI) tract have in common an infiltrate of eosinophils into the wall of the GI tract—sometimes located in the lamina propria only, sometimes in the muscularis propria, sometimes in both. The associated disorders are highly variable in severity of symptoms and endoscopic and histologic manifestations (Table 411-1). Different parts of the GI tract may be involved separately or together (eg, eosinophilic esophagitis is almost always a stand-alone disorder; eosinophilic gastritis may occur on its own, or, more commonly as a gastroenteritis; eosinophilic colitis may occur alone, or in combination with small bowel involvement, ie, enterocolitis). Complicating this is the fact that eosinophils are found in the GI tract in a number of other disorders, not considered to be primarily allergic in origin. These include disease induced by parasitic, bacterial, and viral pathogens as well as certain systemic diseases such as vasculitis. The general principles, diagnostic approach, and management of food allergy is discussed in detail in Chapter 194. 
Table 411-1. Allergic and Eosinophilic Gastrointestinal Disorders
 EPIDEMIOLOGY
EPIDEMIOLOGY
The incidence of food allergies is on the rise and affects 2% to 7.5% of children in the first 3 years of life.1,2,3 During the first year of life, cow milk proteins are the main food antigens involved in GI allergic reactions with an incidence ranging from 0.3% to 7.5%.4 The incidence and prevalence of specific gastrointestinal presentations of food allergy or eosinophilic gastroenteropathies are unknown. Eosinophilic disorders of the intestine appear to be more frequent in children with other immunologic disorders or those receiving immuno-suppression.5,6
 PATHOPHYSIOLOGY
PATHOPHYSIOLOGY
Allergic gastrointestinal disorders can be divided into those that are IgE mediated and those that are not. These disorders are further discussed in Chapter 194. 
The etiology of other eosinophilic gastrointestinal disorders is unclear, as are the relationships to specific food allergens, which are often never identified. Some of these disorders may represent primary immunoregulatory disorders, but a subset of the eosinophilic gastroenteropathies are responsive to food elimination, and these most likely will be due to cell-mediated or IgE-antibody-mediated processes.7
 CLINICAL PHENOTYPES OF ALLERGIC AND EOSINOPHILIC GASTROINTESTINAL DISEASE
CLINICAL PHENOTYPES OF ALLERGIC AND EOSINOPHILIC GASTROINTESTINAL DISEASE
Food Protein-Induced Enterocolitis Syndrome
Food protein-induced enterocolitis syndrome (FPIES) is often considered an anaphylactic-like or anaphylactoid reaction because of its rapid onset, high acuity and upper gastrointestinal (GI) symptoms of vomiting and diarrhea, and systemic manifestations of pallor, hypotension, and shock.7,8 However, FPIES is a non-IgE-mediated process that is associated with villous atrophy and lymphocytic inflammation, as seen in celiac disease, rather than the eosinophilic infiltration found in eosinophilic gastroenteritis. Although the small intestine is the usual target of inflammation, FPIES can be more extensive and cause gastritis, intestinal protein loss (ie, protein-losing enteropathy), or colitis (ie, hematochezia).
FPIES presents in various patterns. An acute presentation with vomiting and diarrhea within 1 to 3 hours of exposure progressing to systemic pallor, lethargy, and hypotension is the most worrisome because of the potential for shock resulting from an unobserved challenge.9,10 This condition appears to be uncommon, with only 14 cases being observed by 2 major food allergy centers over a 5-year span.11 A second subacute presentation begins less dramatically following ingestion of an allergen. This makes it more difficult to pinpoint the relationship to specific foods. There is less vomiting but more diarrhea with poor weight gain as a result of loss of small intestinal surface epithelium (villous atrophy) and resultant nutrient malabsorption. In more severe cases, the infant may progress from failure to thrive to chronic acidemia and methhemoglobinemia.12
FPIES usually begins in infants less than 1 year of age. Formula protein hypersensitivity typically develops during the first month of life. Food protein sensitivities typically develop shortly after the introduction of solids.12 Because of its common use as a formula thickener to treat gastroesophageal reflux, rice-induced enterocolitis can begin before 6 months of age.7,8 Common food allergens include egg white, wheat, rice, peanut, and fish, often in combination. Less common food allergens include oat, barley, sweet potato, squash, string beans, peas, chicken, and turkey.13 Symptoms may be provoked by direct consumption of formula protein or indirectly by antigens crossing through breast milk or via the intrauterine route. Although GI symptoms usually predominate, affected infants typically have other coexisting allergic symptoms, especially eczema. Although symptoms of FPIES often subside by 2 to 3 years of age, they can persist in 30% of the toddlers.
Eosinophilic Gastroenteritis
Eosinophilic gastroenteritis (EGE), also known as eosinophilic gastroenteropathy, is a dense eosinophilic inflammation of the gastrointestinal mucosa accompanied by peripheral blood eosinophilia in 75% of those affected.14,15 The disease is relatively uncommon, predominantly affecting boys and young adult men. Signs and symptoms depend upon the depth of involvement, either to the superficial mucosa alone or deeper. The mucosal involvement can induce abdominal pain, vomiting, diarrhea, and growth failure and, in more severe cases, also involve anasarca from protein-losing enteropathy and iron-deficiency anemia.14,15 Deeper muscle infiltration can lead to gastric outlet obstruction.16 Serosal involvement may rarely lead to ascites.
EGE usually involves the mucosa of the stomach (ie, antrum), small intestine, and occasionally extends to the colon.14 From one third to three quarters of pediatric patients have a history of atopic disease (eg, urticaria, eczema, asthma) or food allergy. The majority have elevated peripheral eosinophil counts and positive food-specific skin prick or radioallergosorbent (RAST) tests. The mucosal form typically occurs in toddlers and responds to an elimination diet.17
EGE is categorized based on the depth of eosinophilic infiltration: mucosal, muscular, and serosal forms, and the distribution of the infiltrate in the gastrointestinal tract.18 Eosinophilic infiltration of the muscle layers results in wall thickening and gastric outlet obstruction or intestinal stenosis that can mimic pyloric stenosis or Crohn stricture, respectively. Serosal involvement is rare but can cause eosinophilic ascites, usually without significant gastrointestinal symptoms. Extraintestinal eosinophilia can rarely involve the other organs, including gallbladder, spleen, pancreas, bladder, peritoneum, and pericardium, to induce polyserositis-like pericardial effusions.19 Other rare presentations include acute abdomen, colonic obstruction, and duodenal perforation from ulcer.20,21
Although the cause remains unknown, the common presence of peripheral eosinophilia suggests an allergic etiology and both IgE and non-IgE-mediated mechanisms are thought to be involved.15 Although specific foods have been implicated in some cases, in most cases food elimination does not resolve the symptoms.17,22 Levels of IL-3, IL-5, and granulocyte colony-stimulating factor are significantly increased.23 New evidence suggests that an underlying immune dysregulation may be a contributory factor.6
Eosinophilic Proctocolitis
Eosinophilic proctocolitis (EPC), also referred to as “allergic colitis,” is the most prevalent and benign of all allergic gastrointestinal disorders.14,24,25,26 EPC typically begins at 4 to 12 weeks of age and is more frequent in boys than girls by a 2:1 ratio. The typical presentation is one of painless hematochezia mixed with mucus and occasional diarrhea, but the infants are otherwise feeding and growing well.14,27 The stools contain flecks of blood, insufficient in amount to cause anemia, unless untreated for long periods. Among all infants presenting with hematochezia, approximately two thirds will be expected to have biopsy-proven eosinophilic proctocolitis.25 The approach to the infant with hematochezia is discussed in Chapter 387. The most common protein sensitivities are to either cow milk (via direct consumption or transfer via breast milk) or soy proteins in formula. In two thirds of breast-fed cases, cow milk is the offending protein, and its elimination from the maternal diet is effective treatment in over 80%.28,29,30
The mechanism of EPC remains unclear. The early window of susceptibility of between 4 and 12 weeks coincides with a period of increased permeability of the mucosal barrier and immaturity of mucosal immune. Elevated levels of eosinophil cationic protein and platelet-activating factor are found in EPE, but the underlying pathophysiology has not been elucidated.31
Cow Milk-Induced Gastroesophageal Reflux
Gastroesophageal reflux is discussed in Chapter 394. Cow’s milk allergy may play an etiologic role in some cases of patients with significant gastroesophageal reflux.32,33,34 These patients have positive skin prick tests, increased nasal or peripheral eosinophilia, and the presence of circulating anti-β-lactoglobulin IgG. Elimination of cow milk improves symptoms that recur when cow milk is reintroduced. The overlap of this entity and eosinophilic esophagitis requires clarification.
Cow Milk Protein-Induced Constipation
Cow milk hypersensitivity appears to induce chronic constipation in some patients.35,36,37 These patients have findings of a higher frequency of concomitant rhinitis, eczema, and bronchospasm, and elevated IgE to cow milk antigens than those with constipation from other causes. The mechanism by which cow milk proteins induce altered colonic function is unclear.
Cow Milk Protein-Induced Anemia
Occasionally, children present between the ages of 1 and 3 years with profound microcytic anemia (hemoglobin 6–8 g), hypoalbuminemia, and excess cow milk intake. Despite the evident pallor and edema on examination, because of its insidious development of anemia and hypoalbuminemia, the child does not develop orthostatic hypotension or symptoms.38 Laboratory studies reveal a profound microcytic anemia, a low serum albumin, and elevated fecal α1-antitrypsin excretion indicating severe iron-deficiency anemia and protein-losing enteropathy. However, stool guaiac test for blood is negative. The dietary history usually reveals that this “milk” baby is drinking in excess of 32 ounces of whole milk largely to the exclusion of other iron-containing nutrient sources. Although full exclusion of cow milk protein, intake of a regular diet, and supplementation with iron is the usual therapeutic approach, one study demonstrates that reduction in cow milk intake below 24 ounces per day rather than total elimination may be sufficient.39 Although the mechanism by which cow milk induces the anemia is unclear, the lack of documented stool heme and threshold effect for milk intake suggests that it more likely results from either iron deficiency or mucosal toxicity rather than from hypersensitivity to cow milk protein.
 DIAGNOSTIC APPROACH
DIAGNOSTIC APPROACH
A positive oral food challenge remains the definitive gold standard test for food allergy.40 However, given the inherent risks involved in those with severe symptoms, such testing may be avoided if alternative nutrient sources are acceptable. If performed, it is recommended that the challenge be carried out in hospital with intravenous fluids and available epinephrine, diphenhydramine, and methylprednisolone. The oral challenge includes progressively increasing (by 2- to 5-fold) amounts of protein every 15 minutes beginning with mg amounts of food protein as described above. Clinical symptoms may be accompanied by a rise in peripheral and stool polymorphonuclear cells.12,41 The challenge is terminated if clinical symptoms occur (vomiting, diarrhea, hypotension, listlessness) or physiologic amounts (2 ounces of formula or 15 g food) of protein have been ingested without symptoms.
Despite its acute presentation, FPIES is a non-IgE-mediated condition, and skin prick and RAST testing are usually negative. Diagnosis is based upon the typical history combined with typical endoscopic findings that include inflammation and villous atrophy, often indistinguishable from that of celiac disease.
Diagnosis of EGE is based upon the clinical presentation and findings of endoscopic evaluation. Laboratory findings of eosinophilia, increased serum IgE, hypoalbuminemia, and protein-losing enteropathy (elevated stool α1-antitrypsin level) are common. Diagnosis requires the demonstration of significant tissue eosinophilia in submucosa (and muscularis mucosa) of the gastric antral and duodenal specimens.42,43 In a few, a lacy mucosal pattern called areae gastricae can be visualized on a barium contrast study.44 The differential diagnosis of gastroduodenal eosinophilia includes Crohn disease, ulcerative colitis, parasitic infections, Ménétrier disease, chronic granulomatous disease, collagen vascular disease, and hypereosinophilic syndrome (ie, hyper-IgE syndrome).
The diagnosis of eosinophilic proctocolitis in infants, and other cow milk allergic presentations, is made based upon the typical symptom presentation and response to removal of the offending antigen. If the child responds promptly to the dietary antigen elimination, no testing is necessary. However if the symptoms persist beyond 4 weeks, a full evaluation should be undertaken. This includes a hemoglobin, stool bacterial cultures, and flexible sigmoidoscopy. The visual sigmoidoscopic findings typically show patchy erythema with friability and edema (mucosal pallor) and occasional mucosal erosions or ulcerations, but in some cases the mucosa may have lymphonodular hyperplasia or may appear entirely normal.31 The histopathology reveals eosinophils (≥ 6/hpf) within the lamina propria and infiltrating normal colonic glands.14,45 Stains for stool polymorphonuclear cells and eosinophils may be positive, but their absence does not exclude EPC. The differential diagnosis includes bacterial colitis, anal fissure, and, much less commonly in infants, inflammatory bowel disease. Most of the infants will outgrow this sensitivity and become tolerant of the offending protein by the age of 1 year. The parents can be reassured about the good prognosis. However, a formal challenge in a physician’s office is recommended to exclude the possibility of evolution to FPIES or anaphylaxis.
A time-limited, 2-week treatment trial of directed dietary elimination may be an appropriate initial diagnostic test in food protein-induced proctocolitis and cow milk–induced constipation.
 TREATMENT
TREATMENT
Treatment of food allergy syndromes requires fastidious avoidance of the offending food allergen(s). In cases associated with anaphylactic-type reactions, a medical alert bracelet that identifies the allergen, as well as provision and training in the use of an epinephrine injection for initial home management of an acute anaphylactic reaction is appropriate. For infants and young children with cow milk protein hypersensitivities, the appropriate choice of a milk substitute should meet certain essential criteria that include no or little cross-reactivity with cow milk, lower allergenicity, and nutritional adequacy. Infant formulas that meet those requirements include cow milk protein (eg, casein, whey) hydrolysates (eg, ≤ 6 amino acid peptides) and elemental (amino acid) formulas.46,47 Soy protein formulas are not tolerated in all cow milk–sensitive infants because soy protein allergy coexists in 17% to 47%.46,47,48 The unpalatability of protein hydrolysate and elemental formulas (requiring nasogastric feedings) and the high costs may affect compliance. In infants with mild symptoms, a hydrolyzed formula should be used for at least 1 month to allow adequate time for mucosal healing. Delayed-type cow milk and soy protein hypersensitivity with predominantly GI manifestations usually become less severe with increasing age. At 1 year, 2 years, and 3 years of age, 45% to 50%, 60% to 75%, and 85% to 90%, respectively, of children become fully tolerant to cow milk protein, with some 25% continuing to manifest severe IgE-mediated type I reactions to milk.49,50 Reintroduction of cow milk or soy protein in a previously highly sensitive child should be performed under medical supervision because of the low but potential risk of anaphylaxis.
Treatment options of children with eosinophilic gastroenteritis include both dietary elimination of food antigens and anti-inflammatory medications and mast cell stabilizers. As first-line therapy, exclusion of the offending food anti-gen(s) either by an elemental diet or elimination diet directed by results of allergy testing or by avoidance of highly allergenic (eg, 6 food elimination) foods can be initiated.17,22 Different from EE, the majority of children have a nonfood-allergic form that responds only to glucocorticoid therapy22 that is associated with side effects, including cushingoid appearance, acne, hirsuitism, impaired growth, and diminished bone density. Although the steroid side effects can be reduced with alternate day or low daily dosing, both can lead to impaired linear growth. Another alternative is budesonide, a corticosteroid that, because of a first-pass liver clearance, has few systemic side effects.51 A number of other classes of medications have been tried with some success. These include mast cell stabilizers cromolyn sodium52 or ketotifen,53 selective leukotriene receptor antagonist,54 and a Th2 suppressor suplatast tosilate.53,55 EGE appears to be a long-standing disorder that is not outgrown with age. Recent trials indicate that an anti–IL-5 antibody (mepolizumab) may be highly effective in patients with steroid-resistant disease.56
 PREVENTION
PREVENTION
Exclusive breastfeeding during the first 6 to 12 months of life has been reported to either prevent or delay the onset of allergic gastrointestinal disease in some studies, but others have not shown similar results. There is limited evidence that feeding with a hydrolysed formula compared to a cow milk formula reduces infant and childhood allergy and infant cow milk enterocolitis.57 Thus, the role of exclusive breastfeeding in preventing food allergy remains somewhat controversial.58 The American Academy of Pediatrics recommends delaying introduction of solids to beyond 6 months of age. For those at high risk for developing food hypersensitivities, based on family history, the American Academy of Allergy, Asthma and Immunology (AAAAI) and the American College of Allergy, Asthma and Immunology (ACAAI) further recommend delaying introduction of cow milk to 1 year, soy, egg white, and wheat until 2 years, and tree nuts and fish until age 3.59 No maternal dietary restrictions during pregnancy are necessary with the possible exception of excluding peanuts.59
REFERENCES
See references on DVD.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


