Alimentary Tract Duplications
Alimentary tract duplications have been described for hundreds of years and multiple terms have been used in the literature. The current term duplication of the alimentary tract and a common description of the congenital malformation was applied by William Ladd in 1937.1 Three common findings were described: a well-developed smooth muscle coat, an epithelial lining, and attachment to the alimentary tract. The first large series to appear in the literature by Gross et al. in 1952 supported these findings as well.2
Embryology
The incidence of duplications has been reported to be 1 in 4500 births.3 Two types are encountered: cystic and tubular, with cystic being the most common. Duplications are considered congenital malformations thought to arise from disturbances in embryologic development. Multiple theories have been postulated to account for their development. A persistent embryonic diverticulum from the alimentary tract was the first theory reported in the literature4, while a defect in the recanalization of the lumen of the alimentary tract was proposed years later.5 The coincidental finding of colonic and genitourinary duplications and similar findings in conjoined twins led to the partial twinning theory.6,7 The ‘split notochord’ theory was proposed because of the association of enteric duplications and spinal anomalies8, and relatively recent literature supports the notochord as being important in the development of both foregut and hindgut duplications.9,10 Fetal hypoxia has also been implicated in the development of duplications.11,12
The associated findings of vertebral, spinal cord, and genitourinary malformations as well as malrotation and intestinal atresia suggest a multifactorial process in the development of alimentary tract duplications.2,13,14 No single theory has been described to account for these heterogeneous malformations.
Clinical Presentation and Diagnosis
Alimentary tract duplications present with a wide range of symptoms including abdominal distension and/or pain, obstruction, bleeding, respiratory compromise, or a painless mass. Generally, the symptoms are related to size, location, type of duplication, and presence of heterotopic mucosa. Most (80%) present before 2 years of age; prenatal ultrasound is detecting duplications as early as 16 weeks gestational age.13–15 The majority of duplications are cystic and the remaining are tubular (Fig. 39-1). The jejunum/ileum is the most common location followed by the esophagus (Table 39-1). The epithelial lining is usually native to the surrounding lesion but heterotopic mucosa is found in 25–30% of duplications.14 Gastric tissue is the most common type of ectopic mucosa encountered followed by both exocrine and endocrine pancreatic tissue. Ectopic gastric mucosa may lead to peptic ulceration with subsequent hemorrhage or perforation (Fig. 39-2).
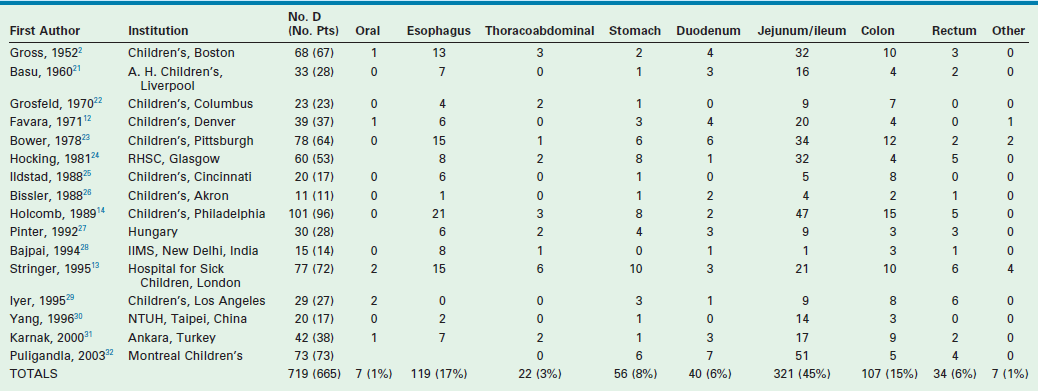
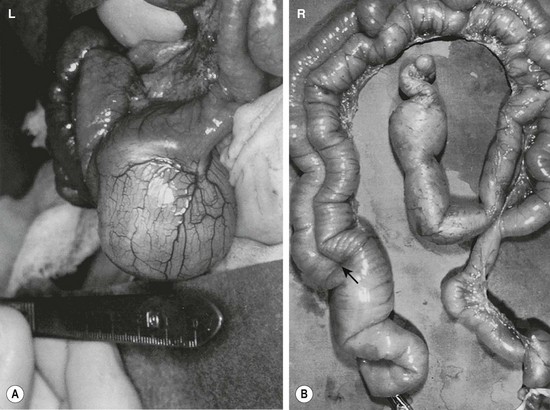
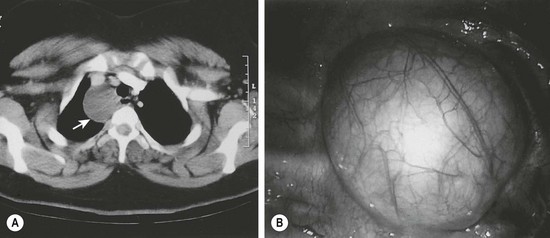
FIGURE 39-1 (A) Most alimentary tract duplications are cystic. (B) A tubular duplication is seen. Note that the native bowel is bifurcated (arrow) into the tubular duplication and native intestine.

FIGURE 39-2 Most intestinal bleeding from duplications is caused by tubular duplications with communication to the intestine. However, in this case, the bleeding was due to mucosal ulceration (solid arrow) secondary to an adjacent cystic duplication. (From Holcomb GW III, Gheissari A, O’Neill JA, et al. Surgical management of alimentary tract duplications. Ann Surg 1989;209:167–74.)
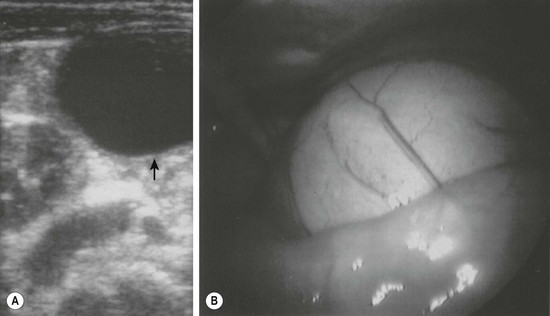
Multiple imaging modalities are utilized to make the diagnosis. Plain radiographs may reveal a mediastinal mass, suggesting an esophageal duplication. Contrast studies may show a mass effect or communication with the alimentary tract. ultrasound is radiation free and noninvasive, making it a useful test, particularly for intra-abdominal duplications.16 A typical sonographic appearance of duplications demonstrates an inner hyperechoic rim of muscosa–submucosa and an outer hypoechoic muscular layer (Fig. 39-3).17 A history of anemia or bleeding with a suspected duplication suggests ectopic gastric mucosa, and technetium-99m (99mTc) scintigraphy is a useful imaging modality.18,19 In cases where a combined thoracoabdominal duplication is suspected, computed tomography (CT) may aid in diagnosis. The presence of vertebral abnormalities and esophageal duplications is best investigated with magnetic resonance imaging (MRI).20
Classification and Treatment by Location
To better understand the wide presentation and surgical treatment of duplications, they will be discussed according to anatomic location. A compilation of major case series reported in the last 60 years from 16 different institutions is seen in Table 39-1.2,13–14,21–32 The report with the largest number of patients described 101 duplications in 96 patients.14
Esophageal Duplications
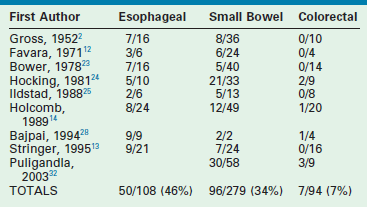
Approximately 20% of duplications arise from the esophagus. While cervical duplications do occur, the majority are located on the right side of the thoracic esophagus. Most are cystic and do not share a common muscular wall or communicate with the esophageal lumen. Clinical presentation will depend upon mass effect. Duplications impinging upon the trachea may lead to respiratory distress or pneumonia. In older patients, dysphagia may develop. Duplications should be in the differential diagnosis for any patient presenting with a mediastinal mass. Almost half of all esophageal duplications contain ectopic gastric mucosa so peptic ulceration leading to anemia or hematemesis can be seen (Table 39-2). Communication with the spinal canal is seen in 20% of patients.14 Once a duplication is suspected on chest radiography or esophagography, further imaging with either CT or MRI should be performed (Fig. 39-4). It is important to evaluate for synchronous abdominal duplications as a 25% incidence has been described.14 With the increased use of thoracoscopy, many esophageal duplications are being resected with a minimally invasive approach rather than the traditional thoracotomy.33,34
Thoracoabdominal Duplications
Extension of an esophageal duplication into the abdomen is known as a thoracoabdominal duplication. These are quite rare accounting for approximately 3% of all duplications. The length of extension can vary from the stomach to the jejunum, with jejunal connections being the most common.13,14
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


