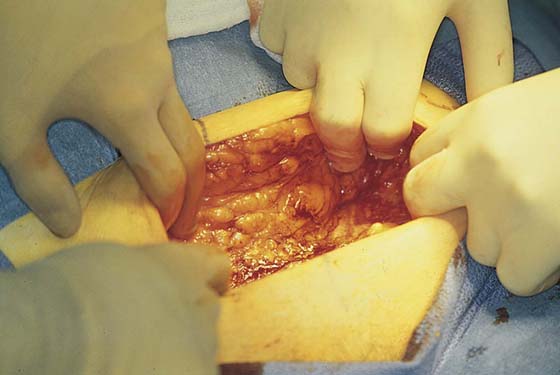
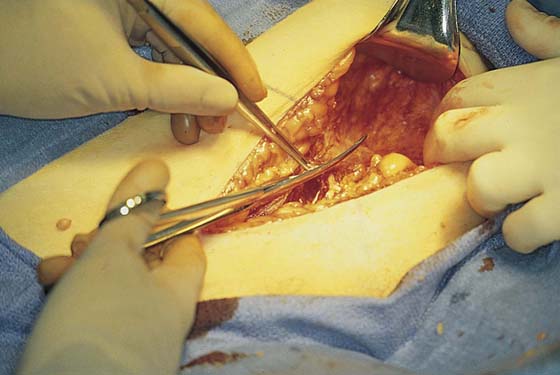
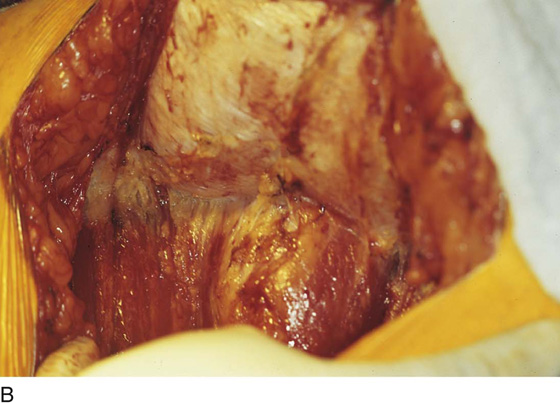
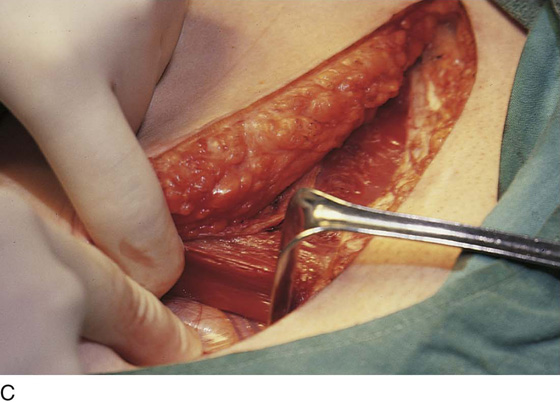
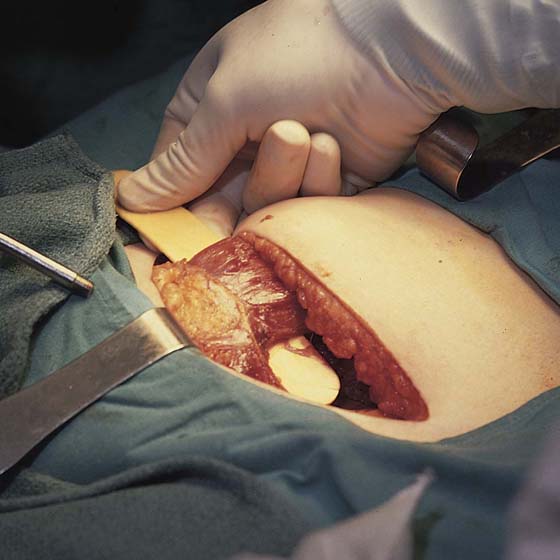
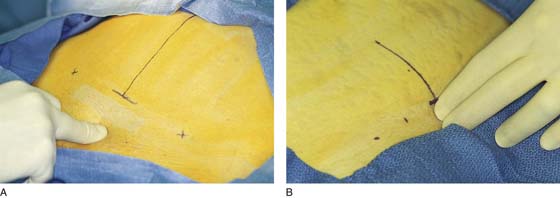
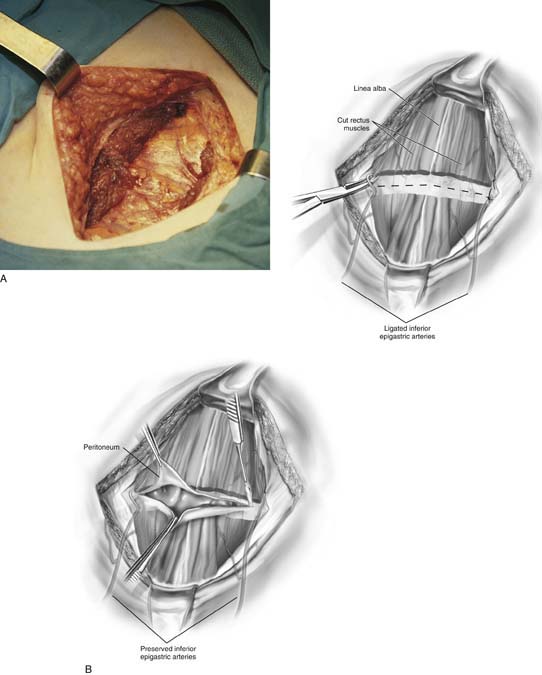
CHAPTER 8 Before performing an incision in the abdominal wall, the gynecologic surgeon should have anticipated the type(s) of surgical procedure that will be done and possible complicating aspects associated with the operation. Consideration should be given to how far cephalad from the pelvis the operative exposure will need to be. Additionally, the surgeon should weigh the cosmetic desire(s) of the patient, the urgency of the surgery, the patient’s history of previous laparotomies, and the risk of postoperative wound dehiscence. Knowledge of pelvic anatomy of the anterior abdominal wall is essential to avoid or secure major vessels, to enhance appropriate repair so as to reduce the risk of incisional hernia or wound dehiscence, and to facilitate smooth entry. Practically, incisions may be categorized as midline or transverse. Transverse incisions may be further subdivided into muscle-splitting and muscle-cutting varieties. The Maylard incision is made two fingerbreadths above the symphysis pubis (i.e., approximately 3–4 cm) (Fig. 8–1A, B). It is carried down through the subcutaneous fat and through Scarpa’s fascia (Fig. 8–2). The fascia overlying the abdominal wall muscles is identified (Fig. 8–3). Scarpa’s fascia covers the sheath of the rectus abdominis muscles and the aponeurosis of the external oblique. The operator should, of course, be familiar with the course of the inferior epigastric vessels, which lie on the transversalis fascia. After taking their origin deeply at the lowest portion of the external iliac artery and vein, the inferior epigastric vessels range anteriorly, cephalad, and medially to cross the lower abdominal wall and locate alongside the rectus abdominis muscles. The fascia overlying the rectus abdominis muscles is cut transversely, and the incision is continued laterally to include a greater or lesser portion of the external oblique aponeurosis (depending on the planned width of the incision) (Fig. 8–4). Next, the fascia is cut in the midline between the two recti (Fig. 8–5A–C). The operator inserts one or two fingers under the rectus muscle from the midline to the right or left, depending on which muscle is to be cut first. The finger(s) emerges from the lateral border under the rectus muscle above the inferior epigastric vessels (Fig. 8–6). The muscle is carefully cut over the operator’s finger(s) or a sterile tongue blade (Fig. 8–7). A similar procedure is carried out on the opposite side (Fig. 8–8A). If the incision is to be extended, the inferior epigastric vessels are isolated, doubly clamped, cut, and suture ligated with 3-0 Vicryl or 2-0 silk. Finally, the peritoneum is elevated, incised, and opened along the length of the incision transversely (Fig. 8–8B). FIGURE 8–1 A. The midline is marked with a solid vertical line. B. The Maylard incision is made 4 cm (two fingerbreadths) above the superior margin of the pubic symphysis, indicated by the dotted line. FIGURE 8–2 The transverse incision is carried deep through the thick fat to Scarpa’s fascia. FIGURE 8–3 The underlying fascia of the rectus sheath is visible at the depth of the incision. FIGURE 8–4 The fascia of the anterior rectus sheath is incised transversely with curved Mayo scissors. FIGURE 8–5 A. The rectus muscle is now clearly in view. B. The lower portion of the rectus fascia (sheath) is dissected from the muscle belly. C. The inferior epigastric vessels are identified. FIGURE 8–6 The linea alba has been incised, and the fingers of the operator’s hand bluntly dissect the muscle from the posterior sheath/peritoneum. FIGURE 8–7 The belly of the rectus sheath is isolated before it is cut. FIGURE 8–8 A. The rectus muscles have been fully divided. Note how dry the field and muscles are even in the absence of any ligatures. B. The schematic view (upper figure) shows the isolation and division of the inferior epigastric vessels and the transverse sectioning of the rectus muscles. The lower figure shows the incision through the peritoneum (in this case preserving the inferior epigastric vessels).
Abdominal Incisions
Transverse Incisions
Maylard Incision


Pfannenstiel Incision

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


