Fig. 52.1
Histological picture of excised bronchogenic cyst. Note the respiratory epithelial lining, seromucinous glands, and cartilage in the wall
Embryology
Bronchogenic cysts result from an abnormal budding of the tracheobronchial tree.
During embryonic development, the primitive foregut arises in the third week of gestation and divides into dorsal portion, which elongates to form the esophagus and ventral portion, which differentiates into the tracheobronchial tree.
Errors in the development of the ventral foregut will give rise to bronchogenic cysts.
Lesions arising before or during the separation of the embryonic foregut are situated in the mediastinum (30 %; Fig. 52.2).
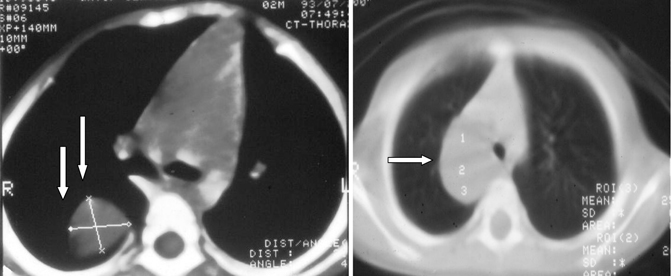
Fig. 52.2
CT scan of the chest showing an intrathoracic bronchogenic cyst and note its relation to the trachea in the second one
Most of these cysts are located close to the trachea near the carina or main stem bronchi and often are attached by a stalk or share a common wall with one of the major airways. Rarely, there is communication of the cyst with the tracheobronchial tree (Fig. 52.2B).
Lesions arising after separations are frequently situated within the lungs (70 %). They are thought to result from abnormal airway branching secondary to defective epithelial/mesenchymal cell interaction during the fourth to seventh weeks of gestation (Fig. 52.3).
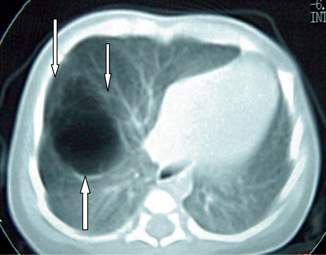
Fig. 52.3
CT scan of the chest showing an intrapulmonary bronchogenic cyst
These intrapulmonary bronchogenic cysts will often communicate with the bronchial tree and about two-thirds of them will be aerated (Fig. 52.4).
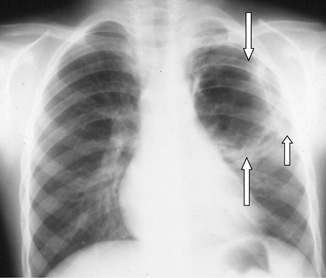
Fig. 52.4
Chest x-ray showing a bronchogenic cyst in the left upper lobe. Note that the cyst is aerated suggesting a communication to the tracheobronchial tree
Intraparenchymal cysts have been consistently reported to be lined by respiratory epithelium and cartilage.
It is possible that accessory buds from the tracheobronchial tree/primitive foregut may get excluded from the thorax and migrates in an unusual manner to lie in abnormal locations.
Sites and Pathology of Bronchogenic Cysts
Bronchogenic Cysts are developmental abnormalities of the primitive foregut.
They arise from an abnormal budding of the tracheobronchial anlage of the primitive foregut during the third to seventh weeks of development.
When attachment to the primitive foregut persists, the cyst is usually associated with the tracheobronchial tree or the esophagus (mediastinal and intrapulmonary bronchogenic cysts).
If complete separation occurs, the cyst may occur in other unusual locations, presumably by migration. These unusual and remote sites include:
Inter-atrial septum.
Neck.
Esophageal wall.
Intrapericardial.
Abdomen.
Cutaneous and subcutaneous tissues.
Scapular region.
Retroperitoneal space.
Bronchogenic cysts have also been reported to extend from the mediastinum through the diaphragm into the abdomen as dumbbell cysts.
Bronchogenic cysts are usually single but rarely may be multiple.
They are lined by columnar ciliated epithelium, and their walls often contain cartilage, smooth muscles, fibrous tissue, and bronchial mucous glands. Occasionally, cysts may contain gastric mucosa (Fig. 52.5).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


