Concern about growth is usually raised when:
- Weight is below the 2nd centile
- Height is below the 2nd centile
- Or when height or weight cross down two centiles.
Growth and weight faltering are common in the first 2 years of life, and expertise is needed to diagnose a normal growth pattern from a pathological cause. There is some debate about the terms used. Weight faltering has replaced failure to thrive and tends to imply that the condition is not serious and is transient. Failure to thrive (FTT) implies not only growth failure, but also failure of emotional and developmental progress. It usually refers to babies or toddlers who have been subject to neglect. The most common causes of weight faltering and failure to thrive are non-organic.
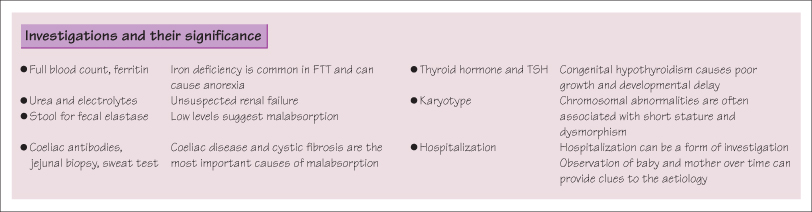
It can be very distressing when a young child’s weight falters, and the evaluation needs to be carried out sensitively. The purpose is to differentiate the child with a problem, and to identify contributing factors whether organic or non-organic (which may coexist). It is important that a normal, healthy but small baby is not wrongly labelled as having a problem. Investigations need to be requested judiciously.
 Weight Faltering Due to Environmental or Psychosocial Causes
Weight Faltering Due to Environmental or Psychosocial Causes
Psychosocial problems are the commonest cause. Problems may include eating difficulties, difficulties in the home, limitations in the parents, disturbed attachment between mother and child, and maternal depression or psychiatric disorder. Uncommonly, neglect is a factor.
Most commonly the child is from a caring home, where parents are anxious and concerned. The problem is often one of eating difficulties, where meals are very stressful and parents do their utmost (often counter-productively) to persuade the child to eat. The picture is quite different from the neglected child who shows physical signs of poor care and emotional attachment. In this case the problem is often denied and compliance with intervention poor.
Management must suit the underlying problem. An organic cause needs to be excluded first. The family health visitor should then be involved for nutritional advice and help with eating problems. Practical support can ease the stress, and nursery placement can be very helpful as well as helping to resolve eating difficulties. Occasionally it is necessary to admit the baby to hospital for observation.
Failure to Thrive
FTT implies not only growth failure, but also failure of emotional and developmental progress. Weight gain is usually first affected, followed in some by a fall in length and head circumference. The child’s development may also be delayed. Where neglect is the cause and the family is not amenable to help, social care must be involved. A minority of children need to be removed from their homes.
Malabsorption
Malabsorption is an important cause of poor weight gain. Diarrhoea and colic are usually present as diagnostic clues. The commonest causes of malabsorption are coeliac disease and cystic fibrosis. In the former, the growth curve characteristically shows fall-off in weight coincident with the introduction of gluten to the diet.
Chronic Illness
Children and babies with any chronic illness may grow poorly. They rarely present as a diagnostic dilemma as the manifestations of the disease are usually evident. However, organic causes may be compounded by psychosocial difficulties and these need to be addressed. Very rarely, chronic disease can be occult and present as weight faltering. In some cases gastrostomy placement may be required.
Familial Causes
Small parents tend to have small children and small, healthy, normal children with short parents should not arouse concern. Usually growth is steady along the lower centiles, but large babies born to small parents may cross down centiles before settling onto their destined line.
Familial Causes
Genetic syndromes are quite commonly associated with short stature, often with congenital abnormalities or dysmorphic features. Intrauterine growth retardation (IUGR) results from adverse uterine conditions that may affect infant growth. When this occurs early in gestation, length and head circumference as well as weight may be affected, and growth potential may be jeopardized. The cause of the IUGR should, where possible, be identified.
KEY POINTS
- Be sensitive. It can be very distressing to parents if a baby has weight faltering or fails to thrive.
- Differentiate significant weight faltering from the normal baby who is ‘catching down’ centiles.
- Identify any symptoms and signs suggestive of organic conditions.
- Only perform laboratory investigations if there are clinical leads in the history and physical examination.
- Identify psychosocial problems that are affecting the baby’s growth and provide appropriate help and support.



