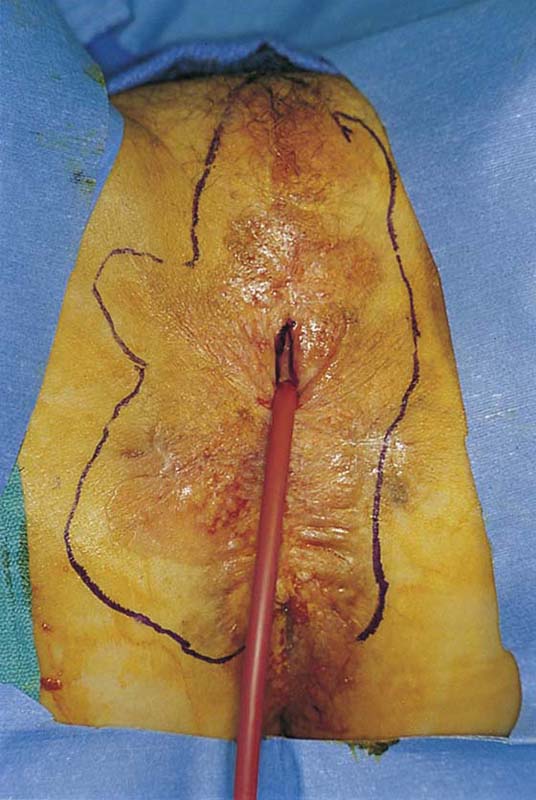
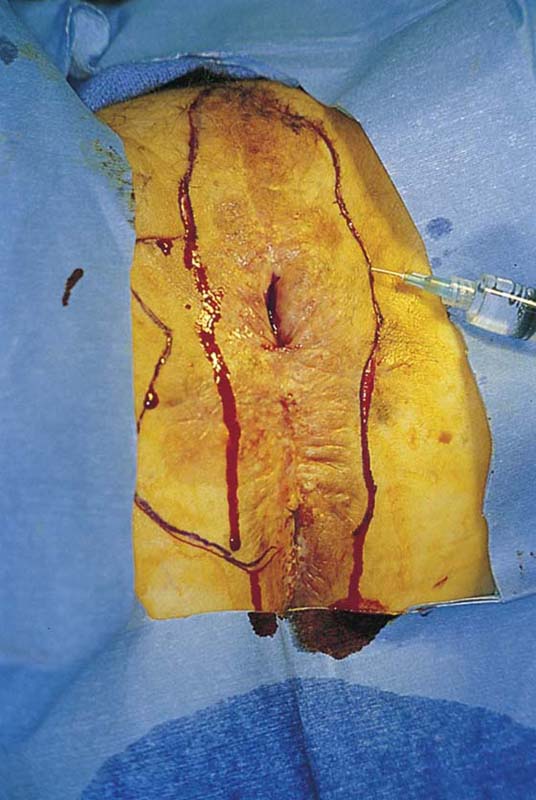
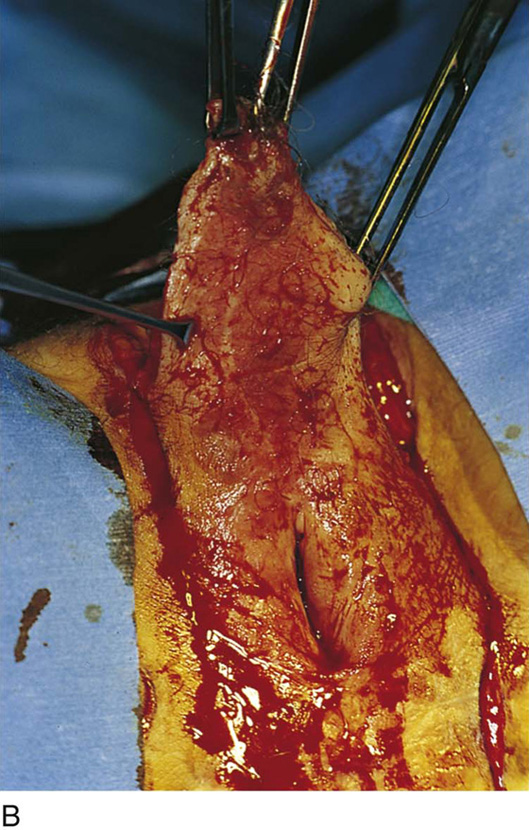
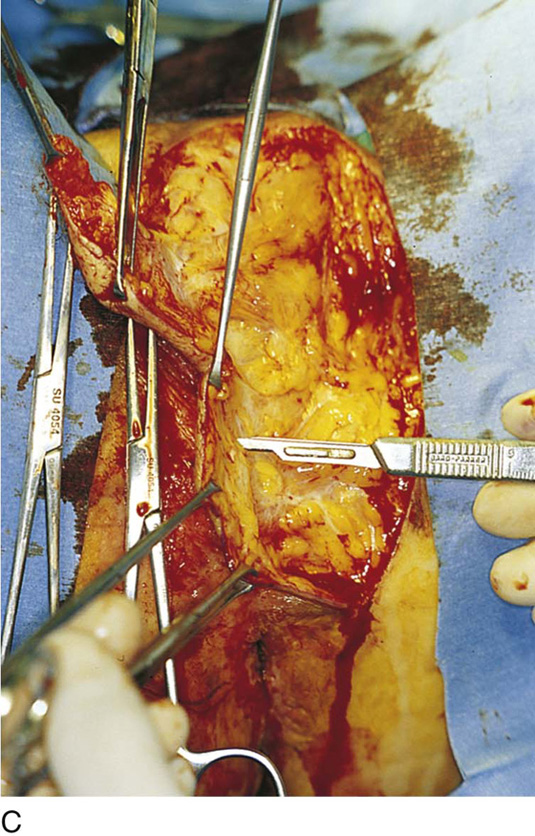
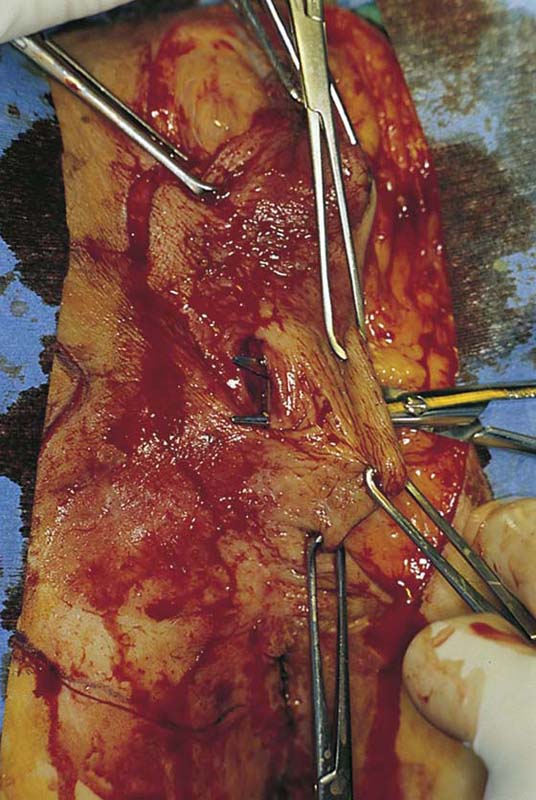
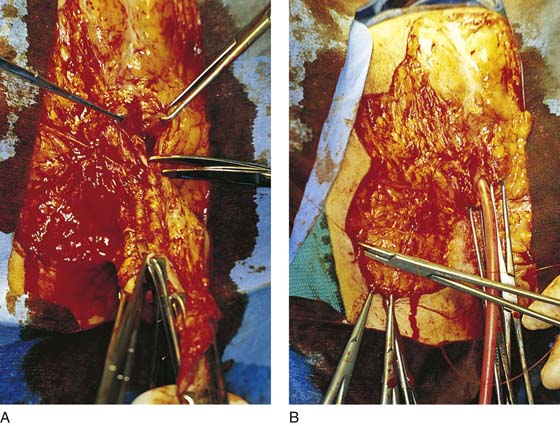
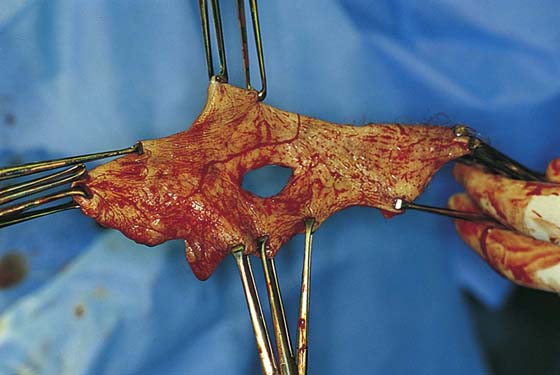
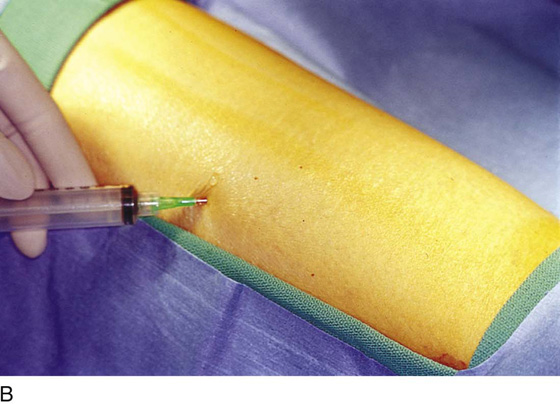
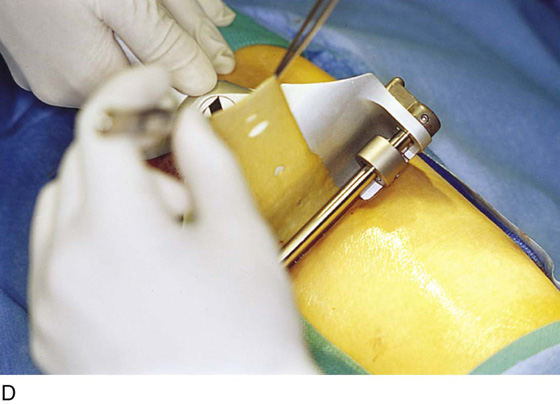
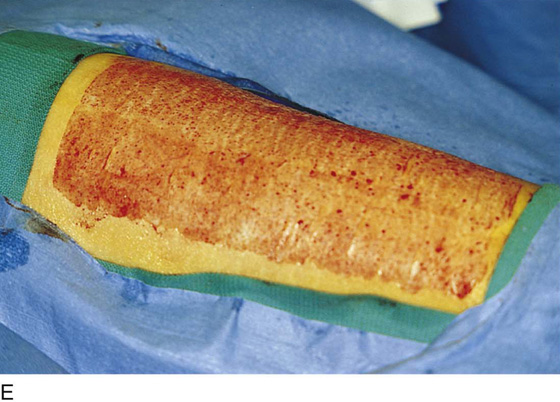
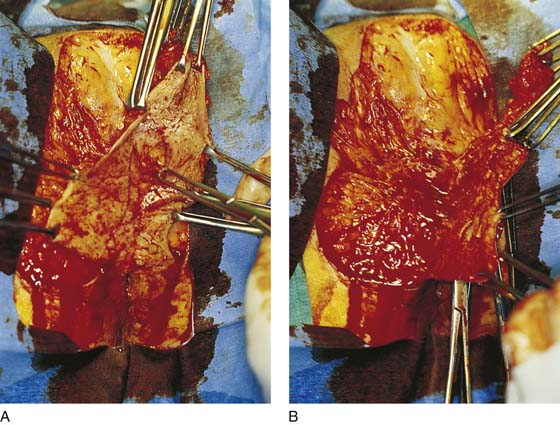
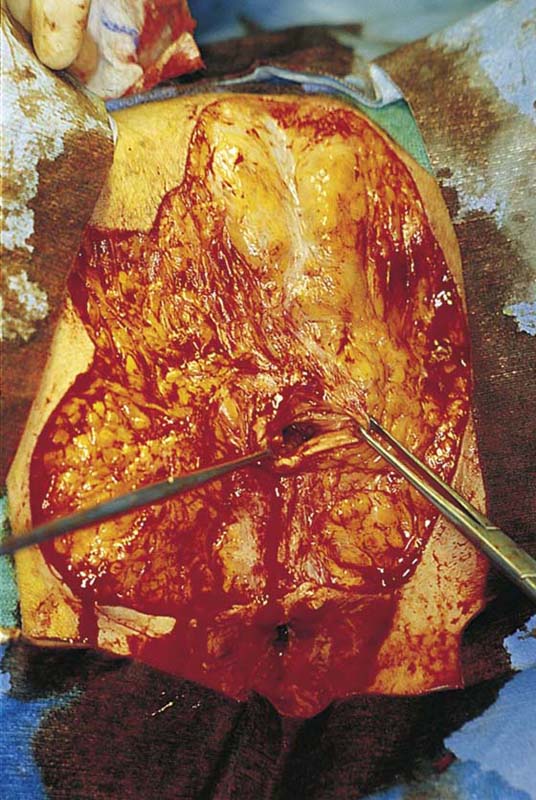
CHAPTER 71 Vulvectomy of any sort is not a simple operation because it destroys an important part of a woman’s normal anatomy and psychologically is a significant blow to the individual’s self-esteem. The vulva is an integral element of feminine sexual anatomy and physiology, and its loss seriously compromises an important day-to-day function. This operation therefore should be performed as a last resort when wide excision, laser excision, or laser vaporization cannot be performed, or when the end result of these procedures would produce a similar outcome—vulvectomy. A modification to simple vulvectomy is “skinning vulvectomy,” which is a shallower excision. Logically, the need for very deep excision for intraepithelial disease is difficult to justify because the average thickness of involved mucosa (hair-bearing areas) ranges from 0.35 to 1.6 mm (mean thickness, 0.93 mm ± 0.37 mm). The depth of involved appendages ranges from 0.43 to 3.6 mm (mean depth, 1.53 mm ± 0.77 mm). Thus an excision of 2 to 3 mm will remove in excess of 95% of involved skin and appendages, predictably eradicating the disease. No justification is known for excising the vulva to a depth greater than 5 mm unless the operation is being performed for invasive carcinoma. The patient is placed in the lithotomy position (not high lithotomy) (Fig. 71–1). After preparation, the extent of the incision should be sketched with a marking pen (Fig. 71–2). The incision is carried down from the lower mons to the lateral aspect of the labium majus with a 3-mm peripheral margin (from the lateral crease of the labium). This is continued to the lowest border of the labium majus, then across the perineum to the opposite side. The incision is brought upward on the opposite lateral margin of the labium to reach the starting point on the mons (Fig. 71–3). A vasopressin 1 : 100 solution is injected along the shallow cut edges of the incision. The incision then is carried into the fat to a depth of approximately 4 to 5 mm (from the surface) (Fig. 71–4A through C). If the clitoris and the labia minora are not involved, they should be preserved. Similarly, if the vestibule is not involved, it should be preserved. The defect created by excision of the labia majora and perineum is covered by a split-thickness skin graft, and a pressure dressing is applied. If the labia minora, vestibule, and clitoris are involved in the intraepithelial neoplasia, then excision should include these structures. The depth of incision should not extend below Colles’ fascia (Fig. 71–5). The dissection progresses from above downward and from lateral to medial (Figs. 71–6 through 71–8A). The body of the clitoris should be preserved. If the hood and glans are involved and have biopsy-proven carcinoma in situ, then the glans clitoris, the sheath, and the frenulum should be excised with the labia minora. The body of the clitoris is never exteriorized to simulate any part of the removed glans. Hemostasis is maintained by clamping off any and all bleeding vessels; this is followed by suture ligation with 3-0 Vicryl (Fig. 71–8B). Electrosurgical coagulation and dissection should be avoided in this area because it devitalizes tissue and increases the risk of necrotizing fasciitis. The dissection is carried to the vaginal margin, which is then circumscribed (Fig. 71–9). The specimen is removed (Fig. 71–10). If primary closure can be accomplished without excessive tension on the suture line, then this type of closure is preferred; otherwise a split-thickness graft should be applied to the defect and sutured medially to the vaginal margins and laterally to the residual skin of the vulva and perineum (Fig. 71–11A through E). Care should be taken not to cause deviation of the axis of the urethra. It is obvious that the surgeon should dissect superficial to the external anal sphincter, perineal muscles, and levator ani muscles during the perineal portion of the vulvectomy. Exposure of muscle indicates that the surgeon has dissected unnecessarily too deep. Unfortunately, these wounds cannot be practically dressed. The operative site should be covered with Silvadene cream 3 times per day and at bedtime when primary closure has been implemented. When a split-thickness graft has been applied, a pressure dressing consisting of fine-mesh gauze (Xeroform) followed by fluffed 4 × 4-inch sterile gauze pads should be applied and remain in place undisturbed for 1 week (Fig. 71–12). A Foley catheter must be inserted because voiding will be impossible (Fig. 71–13). FIGURE 71–1 The patient is placed in the lithotomy position. Pneumatic compression boots have been placed on both inferior extremities. The inferior extremities are lightly flexed and minimally abducted. Neither extremity touches the stirrups. The patient’s buttocks are in firm contact with the operating table. FIGURE 71–2 The vulva is distorted from prior surgery and scar formation. The introitus is shrunken. The vulva shows the characteristic red appearance of Paget’s disease. This diagnosis has been made by preoperative biopsies. A sterile marking pen has traced the outline of the intended excision. FIGURE 71–3 Light scalpel pressure follows the trace pen lines to again outline the boundaries for excision. A 1 : 100 vasopressin solution is injected subdermally. FIGURE 71–4 A. The scalpel cuts deeply at the 12-o’clock location into the subcutaneous fat. The edges of the specimen margins are grasped with Allis clamps, and the tissue is pulled outward and slightly inferiorly to create traction. B. The flap is rapidly developed. Hemostasis is maintained by applying mosquito clamps to any bleeding vessel. The margins of the excision are continuously checked. C. The depth of the excisional tissue plane is approximately 4 to 5 mm. Traction and countertraction are exceedingly important to ensure uniform thickness of the tissue that is to be removed. FIGURE 71–5 The entire upper half of the vulva has been separated from the underlying connective tissue. FIGURE 71–6 An incision is made circumferentially around the lower vagina. The vestibule is cut away together with a 5-mm margin of lower vagina. FIGURE 71–7 A. The lower right side of the vulva is dissected to the level of the anal verge. B. The lower left side of the vulva is dissected to the level of the anus. FIGURE 71–8 A. The last connections of the vagina to the vulva are cut. B. The specimen has been removed. Bleeding sites are sutured (figure-of-8 suture) with 3-0 Vicryl. FIGURE 71–9 The vagina is grasped with Allis clamps, and the margins are closely evaluated for adequacy. FIGURE 71–10 The specimen is oriented and sent to pathology. The author prefers to wrap the specimen in a saline-soaked sponge and transport it immediately to the gross pathology laboratory.
Vulvectomy
Simple Vulvectomy





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


