On successfully completing this topic, you will be able to:
decide when an instrumental delivery is appropriate
decide which instrument is most appropriate in a specific circumstance
appreciate the techniques required for vacuum and forceps delivery
recognise and appreciate the causes of failure to deliver with the instrument selected
know what to do when the instrumental delivery has failed.
Introduction
Operative vaginal delivery (OVD) aims to expedite the delivery of a baby who is believed to be at risk of compromise or when the mother is unable to push it out herself. Worldwide, assisted vaginal delivery remains an integral part of the obstetrician’s duties. Rates vary from 1.5% of deliveries (Czech Republic) to 15% (Australia and Canada) and from 9% to
13% regionally in the UK. These varying rates reflect not only different clinical practices but also different attitudes. Low OVD rates may reflect high CS rates, including those performed at full dilatation, because of a reluctance to perform instrumental deliveries. There is evidence of an increasing trend towards using emergency CS directly for delay in the second stage, without resort to a trial of instrumental delivery. This is particularly with occipito-posterior positions at midcavity. Although instrumental vaginal delivery can be hazardous and should be undertaken with care, the difficulty of CS at full dilatation should not be underestimated; it can be extremely difficult and is associated with high maternal morbidity. There is emerging evidence to support the direct supervision of trainees in this situation in order to maximise the appropriate number of operative vaginal deliveries both attempted and achieved.
Women who labour are, by definition, aiming for vaginal delivery and therefore efforts should be focused on helping them to achieve this normally and safely. Various techniques may help in achieving high spontaneous vaginal delivery rates, such as the use of a partogram, companionship in labour, delaying pushing in women who have had epidural anaesthesia, upright posture and active management of the second stage of labour using oxytocin in nulliparae with epidurals.
Training and simulation in obstetrics
Simulation has an increasing role in developing appropriate skills for OVD. Use of ‘high fidelity’ manikins such as the PROMPT pelvic simulator, can allow objective assessment of traction force. Dupuis et al. have shown that sophisticated simulators can accelerate gaining competence in accurate forceps application (using computer-aided tracking technology).1
Importance of nontechnical skills in OVD
Bahl et al.2 initially described the ‘technical skills’ required to undertake an operative vacuum delivery and described three ‘skills’ covering the areas of:
assessment and preparation
cup application
traction with the cup.
These are particularly useful in teaching trainees, both on simulators and in early patient contact. In their subsequent paper, they outline the vital importance of ‘nontechnical skills’ which include:
situation awareness
decision-making
task management
teamwork/communication
appropriate professional behaviour
crossmonitoring of performance.
It is often errors in these areas that compromise patient safety – one example being loss of situational awareness with an inappropriate number of pulls to try and achieve vaginal delivery. The experienced operator should consider how they teach these skills to their trainees.
Indications for OVD
Indications are:
delay in the second stage of labour
fetal compromise in the second stage of labour
maternal conditions that require either a short second stage or avoidance of Valsalva.
Prerequisites for OVD
Clinical examination should include both abdominal palpation and vaginal examination:
preferably, the fetal head should not be palpable abdominally (i.e. 0/5 palpable); an experienced clinician can consider OVD if the head is no more than 1/5 palpable (this is usually associated with midcavity arrest and malposition)
the cervix should be fully dilated
the vertex (bone, not caput) should be at or below the ischial spines
the exact position of the fetal head should be established
the pelvis should feel adequate clinically.
Informed consent is needed: check that the mother understands and agrees with your plan. The RCOG (2010) has produced advice on consent for OVD.3 The guideline paper outlines which risks should ideally be discussed (within the constraints of the individual clinical situation). A model consent form is provided in the guideline.
Adequate analgesia is needed but this will vary according to the type of delivery proposed, as discussed below.
Make sure the woman is sitting up and tilted as far as practicable to minimise aortocaval compression during the procedure – ideally this should be towards her left side (this is best achieved by placing a wedge underneath her right hip).
Someone should be in attendance that is capable of performing neonatal resuscitation. The operator must be appropriately experienced and skilled.
Safety matters and choice of instrument
When an assisted vaginal delivery is contemplated, careful clinical assessment is vital in order to confirm whether it is appropriate to proceed and to select the most suitable instrument. The different types of ventouse and forceps instruments both have their advantages and disadvantages. Promoting one type over another is inappropriate, as the instrument most suited for the situation at hand, with which the operator is experienced and skilled, is what matters to each individual mother and baby. The advantage of the ventouse cup over forceps relates to its being associated with significantly less maternal trauma and requiring less analgesia, but it is more likely to cause fetal cephalohaematoma and retinal haemorrhage. In addition, ventouse deliveries are significantly more likely to fail than forceps deliveries. Both forceps and vacuum deliveries are associated with an increased risk of shoulder dystocia, but the risk is highest with vacuum (3.5% versus 1.5%). Using a combination of instruments is associated with increased complications. It is best to choose one likely to achieve success.
Different types of ventouse and forceps instruments are available to deal with lift out and rotational deliveries, but the rotational deliveries require particular skills, especially when using forceps. Use of Kjelland’s forceps has declined because of concerns about the risks of increased neonatal and maternal morbidity. However, in skilled hands and following appropriate training and supervision, the overall rates of morbidity are low and can avoid the trauma associated with CS at full dilatation. Recent observational data suggests that the risk of third/fourth degree is no higher with Kjelland’s forceps than with nonrotational forceps (although both have a higher risk than vacuum delivery). Whichever instrument is selected, the operator must be experienced and skilled in its use (or be supervised directly by someone who is). In all cases, as mentioned above, the exact position of the baby’s head must be established before proceeding. There have been many publications over the past 5 years confirming that ultrasound assessment in the second stage of labour allows more accurate confirmation of fetal position. This technique is particularly useful when there is marked caput and can be used as an adjunct (rather than as a replacement) to careful abdominal and vaginal assessment. The operator should place the ultrasound probe suprapubically and seek to delineate the prominent orbital ridges. Ultrasound has also been used in labour to measure degree of asynclitism and descent, as well as predicting the likelihood of achieving a vaginal delivery. It is universally acknowledged that the tendency to put a ventouse on a baby because the position is not clear is totally unacceptable and dangerous. One study demonstrated that 17 of 64 (27%) fetal head positions diagnosed clinically on digital vaginal examination were incorrect when checked with ultrasound and continued vigilance, training and supervision in this area is urgently needed.
Conditions where ventouse should be preferred to forceps
1 Urgent delivery required with no previous analgesia when a low lift out, easy delivery is anticipated.
2 Low lift out delivery, especially if there has been no prior analgesia.
3 Rotational delivery, if operator has inadequate experience with Kjelland’s forceps.
4 Operator or maternal preference, when either instrument would be suitable.
Conditions where forceps should be preferred to ventouse
1 Face presentation (an absolute contraindication to ventouse).
2 Aftercoming head of the breech.
3 Marked active bleeding from a fetal blood-sampling site.
4 Gestation of less than 34 weeks (between 34 and 36 weeks the ventouse is ‘relatively’ contraindicated).
5 Large amount of caput.
6 Certain fetal or maternal haematological conditions (e.g. autoimmune thrombocytopenia [AITP], haemophilia).
7 Mother who is unable or unwilling to push.
Ventouse/vacuum
There are a number of soft cups in common use which are smoothly applied to the contour of the baby’s head and do not develop a ‘chignon’. The vacuum achieved is particularly poor when soft cups are applied to moderate or severe caput (as adhesion to folds of oedematous skin is poor). In addition, they have limited manoeuvrability and cannot be correctly placed when the head is deflexed. Consequently, soft cups have a poorer success rate than metal cups, but are less likely to be associated with scalp trauma. Being soft, they are easy to apply and unlikely to injure the mother. As they are cleaned and sterilised as one item, they present no problems with assembly or leakage.
The hard cups are traditionally metal, the most widely used being the ‘Bird-modification’ cups. These have a central traction chain and a separate vacuum pipe. The anterior cups come in 4, 5 and 6cm sizes. The posterior cup is 5cm in diameter and has either the standard chain or the new cord for traction. The posterior cup is designed to be inserted higher up in the vagina than the anterior cups, to allow correct placement when the head is deflexed. Many units will use the ‘Kiwi’ omnicup cup (a light, disposable, hard plastic cup with integrated vacuum mechanism). A variant has an additional display which allows semi-objective estimation of traction force applied. These cups are useful for both rotational and nonrotational deliveries, but operators should be aware that two studies have suggested a higher failure rate compared with standard metal cup ventouse. Experienced operators usually recommend use of the largest metal cup available when trying to achieve delivery from transverse or posterior positions at pelvic mid-cavity level (i.e. from ‘0’ to ‘+2cm’ below the ischial spines).
It has been shown that successful delivery is most likely with the ventouse when the cup is applied over the flexion point, which lies in the midline just in front of the posterior fontanelle. A cup is ideally positioned when it covers the posterior fontanelle with the sagittal suture pointing to the centre of the cup. A well-placed cup will result in a well-flexed head (Figure 30.1), while failure to put the cup far enough back will result in deflexion and a higher chance of detachment and failure.
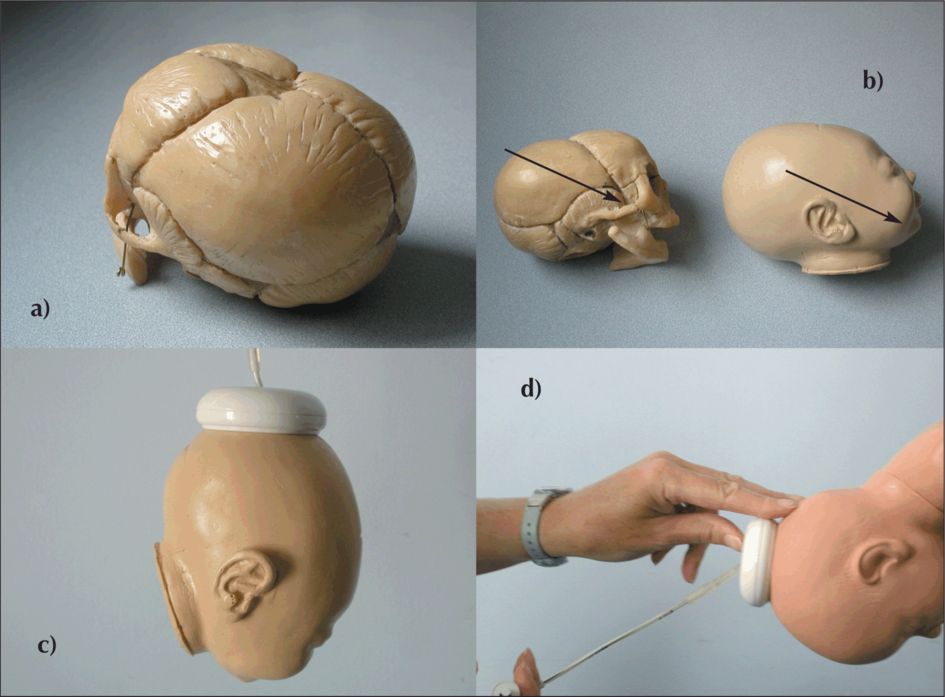
Ventouse: (a) Note how far back the posterior fontanelle is; (b) Note the axis through the flexion point, which results in the smallest presenting diameter; (c) The ventouse cup applied over the flexion point; (d) traction (along the pelvic axis) and the three-fingered grip of the ventouse cup with the second hand.
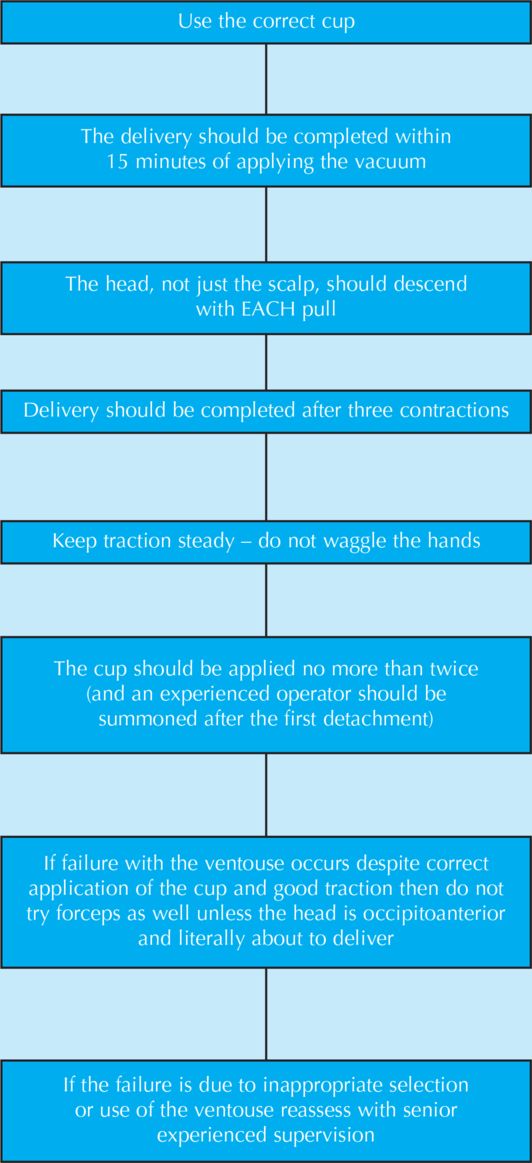
Safe delivery with the ventouse
To minimise the chances of any fetal damage, the basic rules for delivery with the ventouse should be followed. Overall, the risks of perinatal trauma using the vacuum extractor correlate with the duration of application, the station of the fetal head at the commencement of the delivery, the degree of difficulty of the delivery and the condition of the baby at the time of commencement of the procedure. When contemplating using the ventouse, in addition to the factors mentioned above, it is particularly important that there are good uterine contractions and that the mother is fully cooperative and able and willing to push. The increasing tendency to perform operative deliveries in theatre as ‘trials’ (which are conducted under dense regional blockade with associated significant compromise to maternal efforts) may be increasing the likelihood of failures with these instruments.
1 The delivery should be completed within 15 minutes of application of the vacuum (15 minutes is given as the maximum time allowed for application but the average time from insertion of the cup to delivery in over 400 deliveries was 6 minutes).
2 The head, not just the scalp, should descend with each pull.
3 Delivery should be complete within three pulls (if the head is crowning a fourth pull is allowed).
4 Keep the hands steady during traction – do not waggle, as this increases scalp trauma.
5 The cup should be reapplied no more than twice (and after one detachment an experienced operator should be summoned).
6 If failure with the ventouse occurs despite good cup placement and good traction, do not try the forceps as well.
Method
There is no need to catheterise the woman (unless there is another indication, such as epidural anaesthesia). No additional anaesthesia is required (perineal infiltration will suffice if an episiotomy is needed). Lithotomy is the most common position used (and should be used with lateral tilt) but delivery may be possible in dorsal, lateral or squatting positions.
Examine the woman carefully. Estimate the size of the baby by abdominal examination and ensure that the head is fully engaged (less than one-fifth of the head should be palpable). Confirm vertex presentation, position and the amount of caput through vaginal examination. Describe the attitude of the presenting part as ‘flexed’ or ‘deflexed’ (any situation where the anterior fontanelle can be felt easily) and take note of any asynclitisim.
The appropriate cup should be chosen
1 The silicone rubber cup can be used with any well-flexed vertex presentation, as long as the mother is cooperative, the baby is average-sized and there is minimal caput (i.e. by pressing firmly all details of the cranium should be felt, the skin will not be deep and will feel only slightly spongy). This cup is rarely suitable for occipitolateral positions, as the asynclitism associated with them tends to make placement of this cup over the posterior fontanelle difficult.
2 The anterior metal cup should be chosen if the baby is big, if the second stage is prolonged and if there is a moderate degree or more of caput (the skin may feel deep, may be folded and will definitely be spongy). It may also be used if the head is only slightly deflexed or slightly rotated, provided correct cup placement can be achieved. The 6 cm cup is preferable to the 5 cm cup because it allows greater traction without increasing the risk of scalp trauma. Only where the vagina is narrow should the 5 cm cup be used. The small 4 cm cup is reserved for use with the second twin, particularly if the cervix is no longer fully dilated.
3 The most valuable posterior metal cup, as its name indicates, is used for occipitoposterior positions, but also for occipito-lateral positions. It is particularly useful in situations with significant asynclitism and/or deflexion.
Once the correct cup has been chosen and connected to its pump as required (electric or hand) a check should be made for leakages prior to commencing the delivery. Common problems include suction bottles not tightly screwed in or tubing loosely attached to the metal cups (not locked with the small plastic ring). The metal cups should have a meshed bottom plate, which functions to maintain a clear space between the scalp and the cup so that an effective vacuum can be applied.
Silicone rubber cup
The silicone rubber cup is used in the following manner: it is folded and gently inserted into the vagina with one hand from above downwards, while the other hand parts the labia. A gentle twist may help it to unfold into place in the vagina and thereafter it is essentially not manoeuvrable, being larger in diameter than the metal cup and having a relatively inflexible handle.
Take the pressure up to 0.2 kg/cm2, check that no maternal tissue is caught under the cup and then continue directly to 0.8 kg/cm2, beginning traction with the next contraction after this pressure has been achieved. In a recent randomised controlled trial (RCT), there was no significant difference in successful vaginal delivery rates where this method was used (as opposed to sequential pressure increases of 0.2 kg/cm2).4 There were significant reductions in the mean application-maximum negative pressure time (–4.6 95% CI [–4.4 to –4.8]) minutes and in mean application-delivery time (–4.4 95% CI [–4.8 to –4.0]) minutes. Where gentle to moderate traction is required, it is reasonable to take the pressure to 0.6kg/cm2 and in those rare situations where deliveries are undertaken between 34 and 36 weeks, it may suffice to stop at 0.4 kg/cm2.
Traction should be along the pelvic axis for the duration of the contraction. One hand should rest on the bell of the cup (Figure 30.1) while the other applies traction. Malmstrom said: ‘Vacuum extraction is a matter of cooperation between the traction hand and the backward-pressing hand’5. The hand on the cup detects any early detachment and also indicates whether the head moves downwards with each pull. The fingers on the head can promote flexion and can help to guide the head under the arch of the pubis by using the space in front of the sacrum. As the head crowns, the angle of traction changes through an arc of over 90°, but the fetal head should guide the hands, not the other way around: raising the hands too early causes extension of the fetal head, increasing the diameter of the presenting part. This, in turn, increases the risk of trauma to the perineum and can cause cup detachment.
At this point, if necessary, an episiotomy can be cut but if the perineum is stretching as normal, it is simply supported with the hand that was on the bell. Occasionally, an edge of the cup might lift off at the introitus (this is more likely to happen if there is caput present or if the hands have been raised too early). If this occurs, you must be careful not to catch maternal tissue under the cup as it reattaches, and thus this should be rechecked before final delivery of the head.
Anterior metal cup
The metal cup is lightly lubricated and then inserted sideways into the vagina. To orientate the cup, make sure the chain and vacuum pipe lie centrally over the posterior fontanelle. Check that no maternal tissue is included at low pressure then traction can commence once a negative pressure of 0.8 kg/cm2 has been achieved. Otherwise, the controlled two-handed manner of delivery is similar to that described for the soft cup above, classically using the
‘three-finger grip’ for the fingers on the cup and head (Figure 30.1). This not only helps to confirm that the fetal head and not just the scalp is descending but also that the fingers apply a force which opposes the lifting tendency of the upper edge of the rigid cup when pulling downwards earlier in the delivery and which oppose the lifting tendency of the lower edge when pulling upwards at the end of the delivery.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


