We report a case of a woman in whom uterine arterial embolization was performed using absorbable gelfoam particles for control of refractory postpartum hemorrhage. Ten days after delivery, the woman experienced high fever and low abdominal pain. Histologic findings after hysterectomy were consistent with uterine necrosis and acute suppurative myometritis.
Angiographic selective embolization (ASE) is an effective treatment for postpartum hemorrhage (PPH) with a high success rate (range, 85–95%), but a low complication rate (range, 6–7%). The most common side effects are pain and transient fever. Other rare complications include uterine and bladder necrosis, nerve injury, vesicovaginal fistula, and thromboembolic event. Uterine necrosis has been described but with nonresorbable particles in most of cases. In this study, we report a patient of uterine necrosis complicated with acute suppurative myometritis after ASE for PPH by using absorbable gelfoam particles.
Case Report
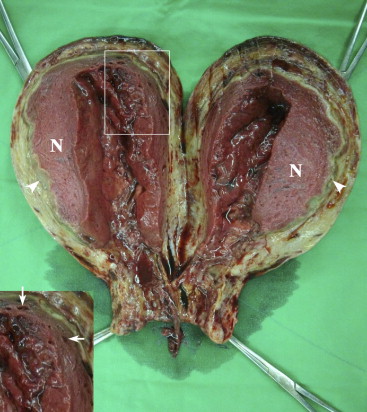
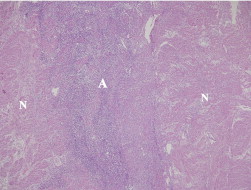
A 38-year-old healthy woman, gravida 2 para 1, was admitted because of labor pain at 39 weeks of gestation. She delivered a 3276 g male infant vaginally with Apgar scores of 6 and 9 at 1 and 5 minutes, respectively. PPH occurred because of uterine atony. Uterotonic agents, followed by uterine packing, were applied but could not stop the bleeding. Therefore, ASE of the uterine arteries was carried out smoothly by injecting gelfoam particles (1-2 mm) (Johnson and Johnson, Skipton, UK). Patient’s condition remained stable after ASE and was discharged without complication 3 days later. Unexpectedly, she suffered from lower abdominal pain 10 days after ASE. Fever was up to 39° C. Physical examination revealed motion tenderness of the uterine cervix and the uterus was at the umbilical level. Under the impression of postpartum fever with endometritis, cefoxitin 2 g every 8 hours was prescribed. Transabdominal ultrasound disclosed a complex echogenicity in the uterine myometrium. Abdominal computed tomographic (CT) scan found air infiltration inside the necrotic myometrium and a peripheral enhancement rim ( Figure 1 ). Along with unrelenting fever and the risk of sepsis, transabdominal hysterectomy (TAH) was performed 14 days after ASE. Gross specimen of the uterus ( Figure 2 ) found a circumferential ischemic necrosis located at inner half of the myometrium and abscess formation in the outer zone of the necrotic region. Histologic examination ( Figure 3 ) showed uterine necrosis associated with acute suppurative myometritis. Bacterial cultures from the abscess revealed heavy colonies of Escherichia coli and Citrobacter koseri . After TAH, she recovered completely.

Comment
Although the hemostatic effect of ASE is excellent for PPH, it is an ongoing challenge to improve the safety of this procedure. Gelfoam is an absorbable embolizing agent commonly used for PPH treatment. After gelfoam embolization, the development of uterine necrosis requiring TAH rarely occurs ( Table ). At least 2 reasons might be related to the occurrence of uterine necrosis. First, the distended uterus after delivery and the lack of anastomosis between uterine and ovarian arteries could cause insufficient blood flow to distal part of the uterus. Second, studies of the ewe suggested that the diameter of the occluded artery was an important factor of uterine necrosis.



