Syndrome
Clinical features
Weyer’s oligodactyly syndrome
Ulnar and fibular ray deficiencies along with midline craniofacial defect such as single central incisor and cleft lip/palate
Cornelia de Lange syndrome (mutation of the cohesion complex)
Ulnar ray deficiency, developmental delay, microcephaly, thick eyebrows meeting at midline, short upturned nose, long philtrum, excessive body hair, visual/auditory abnormalities
Femur-fibula-ulna syndrome (proximal femoral focal deficiency)
Deficiency of ulna, fibula, and femur
Ulnar–mammary syndrome (Schinzel syndrome) (TBX3 mutation)
Ulnar ray deficiency, breast/nipple hypoplasia/aplasia
Langer mesomelic dysplasia (mutation of both copies of the SHOX gene)
Ulnar and fibular ray deficiency, severe short stature mainly to very short legs (mesomelic)
Pillay syndrome (opthalmo-mandibulo-melic dwarfism)
Ulnar and fibular ray deficiency, blindness, fusion of temporomandibular joints
Reinhardt–Pfeiffer mesomelic dysplasia
Ulnar and fibular ray deficiency, shares some of the features of Leri–Weill dyschondrosteosisa
Al-Qattan palmar duplication syndromeb (WNT7A mutation)
Double palm (i.e., the dorsal aspect of the hand has no nails or hair; with the appearance of thick palmar skin on the dorsum), severe lower limb deficiency, variable degree of ulnar ray deficiency
Embryology
Ulnar ray deficiencies occur as a result of deficiency of the Sonic Hedgehog (SHH) (Al-Qattan et al. 2010; Al-Qattan and Kozin 2013). SHH is situated in the zone of polarizing activity (ZPA) within the posterior part of hand paddle. However, SHH diffuses out of the ZPA and acts as a diffusable protein. SHH is considered as the main controller of anteroposterior axis of limb development. Three basic principles should be known regarding this axis of development. Firstly, the normal development of the thumb and radial ray requires the absence of SHH anterior expression and the presence of mesodermal GLI3R/SALL4 and ectodermal FGF8 expression anteriorly. In contrast, the normal development of the fingers and ulnar ray (including the ulnar side of the carpus and ulna) requires a “graded” SHH expression with highest concentration at the little finger and lowest concentration at the index finger. Secondly, any deficiency of SHH will lead to ulnar ray deficiency. In contrast, any overactivity (or increased expression) of SHH will lead to the ectopic anterior expression of SHH, and this will lead to various types of radial polydactyly (Al-Qattan 2013b). Thirdly, maintenance of SHH activity is mediated by two main players: (a) fibroblast growth factor 4 (FGF4) within the posterior ectoderm, known as the FGF4-SHH loop, and (b) the wingless WNT7A protein in the dorsal ectoderm (Al-Qattan 2011). Therefore, in Al-Qattan palmar duplication syndrome (see Table 1), loss of function of the dorsalizing gene WNT7A will not only lead to palmar duplication but also to ulnar ray deficiency (Al-Qattan 2011). Similarly, the main pathology in ulnar-sided cleft hand deformity is suppression of FGF4 within the posterior ectoderm (Al-Qattan 2013a). Ulnar ray deficiency is a common concurrent feature in ulnar-sided clefts because of a defective FGF4-SHH loop (Al-Qattan 2013a).
Ulnar ray deficiency is much less common than radial ray deficiency. Ogino and Kato (1988) explained this by stating that the critical (in utero) period of ulnar deficiency was earlier than that of other abnormalities and it corresponded to a period of high mortality rate of the fetus. The authors also induced ulnar ray deficiency in rats when a teratogen (busulfan) was given between 9 and 10 days of gestation and induced radial ray deficiency when the same drug was given between 10 and 11 days.
Embryologically, the ulnar artery develops before the radial artery and before the development of the ulnar ray (Al-Qattan and Kozin 2013). This explains the findings of Inoue and Miura (1991) who carried out angiography in patients with ulnar ray deficiency and found that the ulnar artery was the main artery to the hand and that 50 % cases had absent or severely hypoplastic radial artery.
Clinical Features and Classification Systems
Patients with ulnar ray deficiency should have complete history and systemic examination to document familial and syndromic cases. Careful clinical and radiological examination of the lower limbs is required since fibular hypoplasia and focal femoral dysplasia are known concurrent features (Fig. 1). Appropriate referrals to the craniofacial team may also be required (see Table 1).
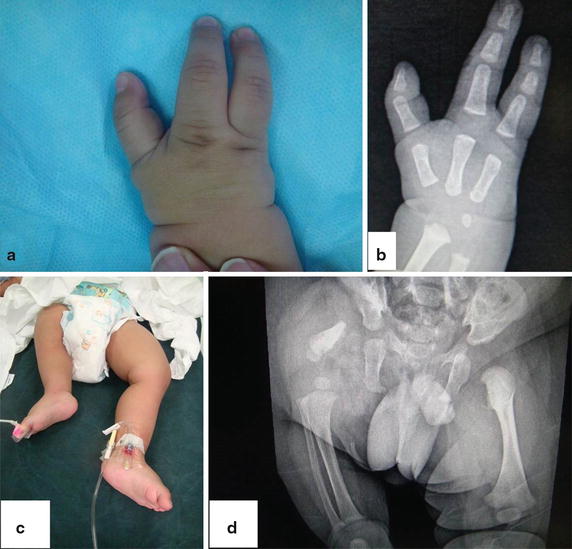
Fig. 1
Unilateral ulnar ray deficiency with ipsilateral focal femoral dysplasia. (a) The hand with absent 2 fingers but excellent function. (b) X-ray of the hand showing a slightly short ulna. (c) The deformity of the right lower limb. (d) X-ray showing the femoral dysplasia. In this case, lower limb management is the priority
The affected upper limb should have full clinical, radiological, and functional assessment (see Table 2). Shoulder instability is rare and was only reported in a single child out of 72 cases of the series reported by Al-Qattan et al. (2010).
Table 2
Assessment/classification/grading of the clinical features of ulnar ray deficiency
Area of interest | Authors | Description/classification |
|---|---|---|
Shoulder | Al-Qattan et al. (2010) | I = stable (normal) shoulder |
II = shoulder instability | ||
Elbow | Kummel (1895) | I = normal |
II = radiohumeral synostosis | ||
III = radial head dislocation | ||
Ulna | O = normal | |
I = hypoplastic ulna | ||
II = partial aplasia of the ulna (distal part) | ||
III = absent ulna | ||
Fingers | Ogino and Kato (1988) | I = little finger hypoplasia |
II = little finger absent | ||
III = absent ulnar two fingers | ||
IV = absent ulnar three fingers | ||
V = absent all four fingers | ||
Thumb/first web deformity | Cole and Manske (1997) | I = normal thumb/1st web |
II = mild deficiency | ||
III = moderate to severe deficiency | ||
IV = absent thumb |
The elbow may be classified as per Kummel classification (Kummel 1895) to identify radiohumeral synostosis (Fig. 2) and radial head dislocation (Table 2).

Fig. 2
Ulnar ray deficiency with radiohumeral synostosis. Note the absent ulnar 3 fingers and the hypoplastic ulna
The ulna may be normal and this was recently stressed upon by Havenhill et al. (2005) and was given the term “type zero ulna.” Ogden et al. (1976) classified abnormalities of the ulna from hypoplastic ulna to absent ulna (Table 2).
Ogino and Kato (1988) provided a classification of ulnar ray deficiency according to the degree of deficiency of the fingers (Table 2). Later, Cole and Manske (1997) stressed on concurrent thumb/first web deficiencies and realized that surgical correction is frequently done for this deficiency. Hence, the authors recommended a separate classification devoted to the thumb (Table 2).
Which Classification System Should Be Used for Research?
This is a controversial issue. Al-Qattan et al. (2010) recommended combining the existing five classification systems shown in Table 2. For example, an affected limb may be classified as shoulder-Al-Qattan type I, elbow-Kummel type III, ulna-Ogden type II, fingers-Ogino/Kato type II, and thumb-Cole/Manske type II.
Lorea et al. (2004) offered more detailed descriptive information about the shoulder, elbow, forearm, wrist, and hand. This may be more comprehensive for research, but it did not gain popularity probably because the identification of the individual features of its five components is via a variety of numbers and letters that are not very workable.
The most commonly used single classification system in scientific papers on ulnar ray deficiency is the modified Bayne classification which is shown in Table 3. The original Bayne classification combines Ogden classification of the ulna and adds a group with radiohumeral synostosis. In the modified Bayne classification, another two groups are added: type O ulna (Havenhill et al. 2005) and the phocomelic type (Goldfarb et al. 2005; Tytherleigh-Strong and Hooper 2003). In 2003, Tytherleigh-Strong and Hooper (2003) noted that some cases were previously diagnosed as phocomelia, but careful examination of the X-rays revealed a radiohumeral synostosis with absent ulna. Hence the proper diagnosis should have been ulnar ray deficiency and not phocomelia. This was later confirmed by Goldfarb et al. (2005) who also noted that this “apparently single” bone occupying the arm/forearm resembled a humerus proximally and a radius distally. This bone will frequently have a large medial epicondyle at the level of what has been the elbow (Fig. 3). These patients are now put in a separate group as type V, Bayne (Table 3). In the genetics literature, the term “apparent” phocomelia of ulnar ray deficiency is used to differentiate it from the “true” phocomelia (Al-Qattan et al. 2013).
Table 3
The modified Bayne classification which is commonly used in clinical series
Classification
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|