Chapter 39 The urinary tract and its relationship to gynaecology
The close connection of the bladder to the vagina and the short urethra give rise to more problems in a woman’s urinary tract than in a man’s. The anatomy of the urinary tract is described on page 343. The function of the urinary tract is to permit waste products of metabolism to be removed from the body in the urinary flow. For this reason the mechanics of micturition will be discussed first.
MECHANICS OF VOLUNTARY MICTURITION
The bladder fills as urine trickles down the ureters. To accommodate the urine the bladder distends, and it can accommodate 300–400 mL of urine without any increase in the resting intravesical pressure, which remains below 10 cmH2O. In the resting state the urethrovesical junction is flat and there is an angle of about 90° between the bladder and the urethra (the urethrovesical angle) (Fig. 39.1A).
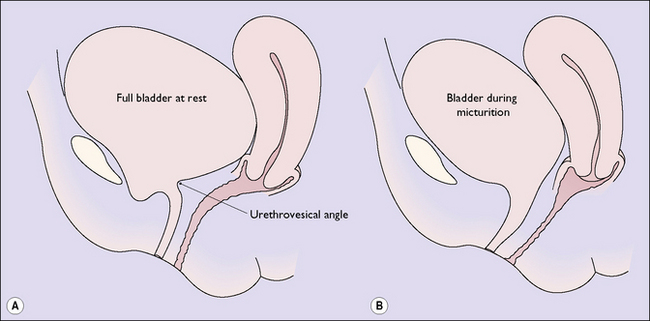
When the person is ready to pass urine the detrusor muscle is permitted to contract strongly, which raises the intravesical pressure above the intraurethral pressure. The detrusor contractions also cause funnelling of the bladder base and obliterate the urethrovesical angle (Fig. 39.1B).
URINARY INCONTINENCE (INVOLUNTARY MICTURITION)
In women two main and two subsidiary forms of urinary incontinence occur. The two main forms are:
The proportion of women complaining of the two main forms of incontinence is not known. The best estimates are shown in Table 39.1.
Table 39.1 Percentage prevalence of the types of urinary incontinence
| Type of Incontinence | Age (Years) | |
|---|---|---|
| <70 | >70 | |
| Urethral sphincter | 50 | 26 |
| Urge incontinence | 20 | 33 |
| Mixed | 30 | 41 |



