CHAPTER 7 The role of electrodiagnosis in infants with brachial plexus palsies
Summary Box
Introduction
Although the task for the electromyographer seems straightforward, accomplishment of the task is often difficult. Traumatic nerve injuries are classically classified into 3 types: neurapraxia, axonotmesis, and neurotmesis. Brachial plexus injuries are complex, and multiple injuries are typically present. The vast majority of persistent lesions are a combination of axonotmesis and neurotmesis. Although the presence of some neurapraxia is possible, it is not the predominate lesion in cases presenting with persistent deficits.1 In 1983, Tassin2 reported the operative series of Gilbert. Of the 100 surgical cases, numerous combinations of involved roots, branches, and trunks were documented. The authors determined that 37 groupings were necessary to classify the injuries. After studying this cohort, only a few consistent patterns emerged from this series. For example, no isolated lower trunk lesions were observed, but rupture of the upper nerve roots/trunk was relatively common.3
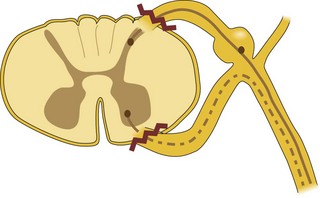
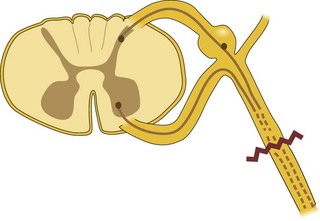
Identification of an avulsed nerve root is important for several reason. Nerve root avulsions are preganglionic lesions. These types of lesions and do not lend themselves to surgical repair (Figure 7.1); however, postganglionic lesions are more amenable to surgical repair (Figure 7.2). The prognosis for recovery of neurological function is unfavorable in preganglionic lesions. When primary repair of the nerve root is not feasible, other surgical options may be available. Preoperative determination that an is present allows the surgeon to determine if surgery is beneficial and to develop a surgical strategy if indicated.
Nerve conduction studies
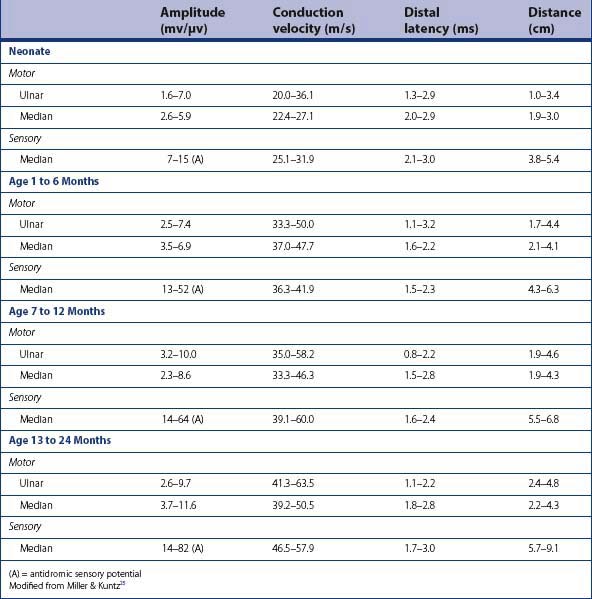
The principles of performing nerve conduction studies (NCS) in the infant and young child are similar to that for the adult patient (refer to Chapter 17) (Figure 7. 3). Due to the infant’s age and size, appropriate modifications must be made (Chart 7.1). It is commonly accepted that the normal values in NCS vary with age (Table 7.1). Motor conduction velocities in newborns are approximately half that of adults (Chart 7.2). Some challenges of NCS in infants exist, such as the difficulty in quantifying axonal loss, and correlating the extent of axonal loss with future recovery.
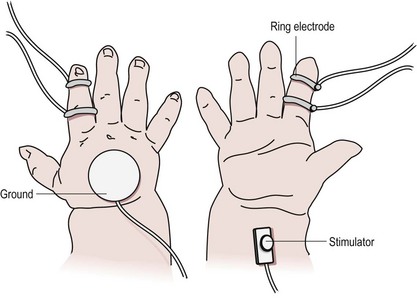
Chart 7.1 Performing nerve conduction studies in infants
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


