Chapter 42 The menopause
From the mean age of 40 (±5) years a woman’s ovaries become less receptive to the effects of follicle-stimulating hormone (FSH) and luteinizing hormone (LH), either because the number of receptor-binding sites on each follicle is decreasing or because increasing numbers of follicles are disappearing, or both. The effect is that oestrogen secretion declines and fluctuates and anovulation becomes more frequent. The fluctuations are a major factor in causing the menstrual disturbances that occur in some women in the years preceding the menopause (see Ch. 28). The negative feedback to the hypothalamus and pituitary gland is less effective, with the result that FSH levels begin to rise. The release of FSH is also increased by the falling levels of inhibin secreted by the ovarian follicles.
The remaining ovarian follicles become increasingly resistant to the higher FSH levels and oestrogen secretion is reduced still further until oligomenorrhoea, and later, amenorrhoea result. If the amenorrhoea persists for 12 months, with or without menopausal symptoms, the menopause has been reached. If the clinician is doubtful whether the menopause has occurred, it can be confirmed by measuring serum FSH on several occasions. A level of more than 40 IU/L indicates menopause (Table 42.1). The measurement of oestrogen levels is not helpful, as the levels of oestrone, oestradiol and oestriol fluctuate even after the menopause, particularly in the first 12 months. A change in the ratio of oestradiol to oestrone occurs, oestrone becoming the dominant circulating oestrogen. After the menopause, any circulating oestrogen detected is synthesized in the peripheral fat by aromatization of androstenedione, derived mainly from the adrenal cortex, with some from the ovarian stroma.
Table 42.1 Postmenopausal plasma hormone levels measured 1 year after the menopause
| FSH (IU/L) | 90 –110 |
| LH (lU/L) | 60 –70 |
| Oestradiol (pmol/L) | 30 –100 |
| Oestrone (pmol/L) | 100 –150 |
| Total testosterone (nmol/L) | 1–3 |
| Free testosterone (pmol/L) | 3–9 |
| Dihydrotestosterone (pmol/L) | 100 –300 |
CHANGES IN THE GENITAL TRACT AFTER THE MENOPAUSE
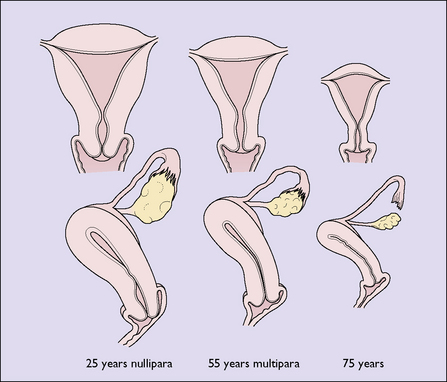
The decline in circulating oestrogen after the menopause leads to atrophy of the organs of the genital tract and the breasts (Fig. 42.1). The ovaries, the Fallopian tubes and the uterus become progressively atrophic. In the uterus, the muscle fibres are converted into fibrous tissue and any fibroids present atrophy. The vaginal epithelium becomes thinner and less rugose, and intermediate cells replace superficial cells. The vaginal secretions diminish, as does the vaginal acidity, and pathogenic organisms grow more easily. The urethral mucosa may become atrophic. In some women, urinary symptoms of frequency, dysuria and incontinence result (see Ch. 39). The pelvic floor muscles lose their tone as their blood supply is reduced; relaxation of the muscles increases and uterovaginal prolapse may become evident (Ch. 38). The external genitals slowly become atrophic, and in old age the labia majora may lose their fat, revealing the labia minora.