Generalized Convulsions
The term convulsion is synonymous with fit or seizure. Convulsions are due to synchronous discharge of electrical activity from a number of neurons, usually with loss of consciousness and abnormal movements. In a generalized convulsion all four limbs and the face are affected. Convulsions are common, occurring in 3–5% of children. They do not necessarily mean the child will go on to develop epilepsy, and many children only ever have one convulsion. However, 60% of epilepsy develops in childhood (Chapter 41). Children’s brains are particularly susceptible to convulsions and the commonest trigger is the rise in temperature during a febrile illness.
Febrile Convulsions
These occur between the ages of 6 months and 5 years in normal children and are triggered by fever, usually as part of an URTI, although they may also be triggered by any febrile illness. They can be simple or complex (see table).
| Simple febrile convulsion (75%) | Complex febrile convulsion (25%) |
| Child age 6 months–6 years | As for simple febrile convulsion but: |
| Single seizure lasting <15 min | Seizure focal or prolonged >15 min, or |
| Neurologically normal before and after | Many seizures occurring in close succession, or |
| Normal neurodevelopment | Status epilepticus |
| Fever not due to CNS infection |
Febrile convulsions should be managed by identifying and treating the source of the fever, and cooling the child by undressing them and sponging with tepid water. Antipyretics such as paracetamol or ibuprofen should be given. If the convulsion persists for more than 10 minutes give anticonvulsants. Status epilepticus (see below) occurs in less than 1% of febrile convulsions. Investigations should be performed to exclude serious infection, and if no obvious focus of infection is found a lumbar puncture is indicated to exclude meningitis.
Advice to parents is very important. About one third of children will have further febrile convulsions in the future. Parents must be taught how to manage fever and basic first aid management of convulsions. The good prognosis should be explained. Children with uncomplicated febrile convulsions are at very little risk of. Overall the risk of epilepsy is 2–3% (about twice the normal incidence). Prophylactic anticonvulsants don’t seem to reduce the risk of future convulsions. If seizures are very frequent a benzodiazepine can be given at the onset of seizure prior to transfer to hospital.
Management of the Fitting Child
Most parents who witness their child having a seizure imagine that the child is going to die and seek medical attention urgently. Children may still be fitting when they present. The most important thing is to support the airway and turn the child into the recovery position, semi-prone with the knee flexed under the chest and the hand under the head. Objects (other than an oropharyngeal airway) should not be put into the mouth. If oxygen is available this should be given by facemask. If the convulsion is ongoing, lorazepam should be given intravenously to terminate the seizure. If intravenous access is not possible, buccal midazolam or rectal diazepam may be used. Occasionally some convulsions persist; this is known as status epilepticus (see below).
It is vital to check blood glucose immediately in any fitting child, as hypoglycaemia is a common and rapidly treatable cause. Not all children with hypoglycaemic convulsions are diabetic; some may have inborn errors of metabolism. Once the convulsion has terminated the child may remain drowsy or ‘post-ictal’ for some time. They should be observed carefully and kept in the recovery position until they are able to maintain their own airway. If it is the child’s first convulsion the parents will require much reassurance and will need to be taught how to manage future episodes. This will include prescribing buccal midazolam or rectal diazepam to be administered at home.
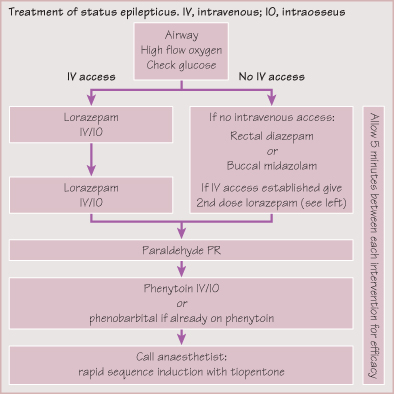
Status Epilepticus
Seizures may be very prolonged and are an important cause of coma. Status epilepticus is defined as continuous seizure activity for more than 30 minutes or a series of seizures without full recovery in between. Status may occur following febrile convulsions or more commonly in children with known epilepsy, or with other acute causes such as trauma or metabolic disturbance. The child’s airway should be opened, oxygen given and blood glucose checked. Anticonvulsant medication should be given as described below. Any child with very prolonged seizures should be monitored carefully on an intensive care unit, and urgent investigations performed to identify the cause.
KEY POINTS
- Febrile convulsions occur in 3% of children between age 5 months and 5 years. The prognosis is usually excellent.
- Children who are fitting must be placed in the recovery position and their airway maintained.
- Always check blood sugar as hypoglycaemia is a common and treatable cause.
- Any convulsion lasting more than 10 minutes should be terminated with buccal midazolam or rectal diazepam.
- Status epilepticus is fitting for more than 30 minutes and requires urgent treatment.



