The Esophagus
Embryologically, the trachea and esophagus are intimately related. The trachea and esophagus both develop from the foregut as a median ventral diverticulum. Familiarity with the embryologic development of the esophagus and trachea is important to understand the congenital abnormalities that arise from these structures. The classic description of these malformations proposes impairment in the process of septation of the trachea and esophagus.1
In humans, normal development of the foregut begins during the fourth week of gestation. At 22 days’ gestation, the foregut endoderm differentiates into a ventral respiratory part and a dorsal esophageal part. The separation of the respiratory part from the esophageal part is achieved by the formation of lateral longitudinal tracheoesophageal folds. The trachea and esophagus elongate first distally and then proximally. At 6 to 7 weeks’ gestation, the separation of the esophagus and trachea is complete. At birth, the esophagus is 8–10 cm in length.2 The length of the esophagus will double in the first few years of life.
Endoscopy
The main value of rigid esophagoscopy in current pediatric practice is for therapeutic procedures such as dilation of an esophageal stricture or removal of a foreign body. Rigid esophagoscopy requires general anesthesia with endotracheal intubation and muscle relaxation. The child is positioned supine with a roll under the shoulders to extend the neck. With care taken to protect the teeth, the esophagoscope, with its bevel up, is introduced into the oral cavity along the hard and soft palates to identify the cricopharyngeus muscle and enter the esophagus. Once the most distal aspect of evaluation is reached, it is easy to examine the esophagus fully when withdrawing the scope to identify any lesions or foreign bodies missed on insertion.
Complications related to passage of a rigid or flexible endoscope are typically at the level of the cricopharyngeus muscle. Perforation of the cricopharyngeus occurs in about 0.093% with flexible endoscopy and 0.074% in rigid esophagoscopy.3 Perforation during diagnostic esophagoscopy is exceedingly rare.
A more thorough description of pediatric esophagoscopy and emerging therapeutic endoscopic techniques can be found elsewhere.4–7
Foreign Body Esophageal Injury
Coins are the most frequently ingested foreign body.8,9 When foreign bodies become lodged in the esophagus, they may cause serious complications. Between 10–20% of foreign bodies may lodge in the esophagus and place the patient at risk for developing complications such as aortoesophageal fistula,10 esophageal perforation,11 esophageal stricture,12 tracheoesophageal fistula,13 and respiratory distress.14 There are four sites of physiologic narrowing in the esophagus: (1) the cricopharyngeus of the UES; (2) the aortic notch; (3) the left main-stem bronchus; and (4) the LES. The cricopharyngeus is the narrowest point in the gastrointestinal tract. Endoscopic removal has been the preferred approach in many referral centers and has been highly successful with low complication rates.
Key principles of endoscopic management of esophageal foreign bodies are to protect the airway, maintain control of the object during extraction, and avoid causing additional damage. Children are more likely than adults to be asymptomatic and have an increased frequency of respiratory symptoms. There should be a high suspicion of foreign body ingestion in infants with excessive drooling, refusal of food, and unexplained coughing or gagging. Anteroposterior and lateral chest radiographs are the best diagnostic tests for radiopaque objects. The flat surface of a coin is best seen on the anteroposterior view when it is lodged in the esophagus, whereas the lateral view will show the flat surface when it is lodged in the trachea (Fig. 26-1).
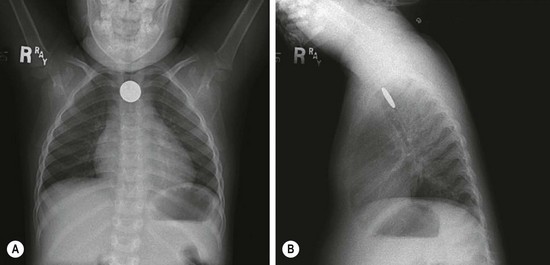
FIGURE 26-1 (A) Anteroposterior and (B) lateral radiographs demonstrate a coin lodged at the cricopharyngeus muscle. Note that coins will most often orient with the flat surface facing anteroposteriorly.
Rigid esophagoscopy has long been considered the gold standard for removal of retained foreign bodies. This procedure has been proven to be highly successful with low complication rates. Other approaches have been described to treat esophageal coins including flexible endoscopy,15 bougienage, 16, 17 Foley balloon extraction under fluoroscopy,8 and brief observation trials.17,18
There is much more concern for serious injury with the ingestion of button batteries. There are four mechanisms of injury caused by batteries: (1) the toxic effect due to absorption of substances, particularly batteries containing mercuric oxide; (2) electrical discharge and mucosal burn; (3) pressure necrosis; and (4) caustic injury from leakage. Severe esophageal damage may occur in as little as four hours after ingestion and perforation in as little as six hours after ingestion.19 Emetics should not be given, owing to their ineffectiveness and possible reflux of a battery back into the esophagus.
There were 20 reported cases of esophageal injury from ingested button batteries from 1979 to 2004.19 Undoubtedly, there are many more unreported incidents. Complications from the ingestion of button batteries include death from vascular invasion and uncontrollable hemorrhage,20 esophageal perforation,21 tracheoesophageal fistula (see Fig. 11-4),22,23 and bilateral vocal cord paralysis.24
Further information about esophageal foreign bodies can be found in Chapter 11.
Chemical Esophageal Injuries
In 2010, the American Association of Poison Control Centers reported that 50% of all human exposures occurred in children under the age of 6 years.25 Household cleaning substances are the third most frequent exposure in children, accounting for 116,000 ingestions per year. In children, ingestions are primarily accidental. The mean age for ingestions is 3.7 years, and 60% of patients are male.26
Caustic injuries are classified similar to burns (Table 26-1). The classification of injury is based on endoscopic evaluation and is used clinically to help predict subsequent clinical outcomes and course. First-degree caustic injuries are superficial and will result in edema and erythema. The esophageal mucosa will slough, but no stricture will form. Second-degree injuries involve the mucosa, submucosa, and muscle layers. They result in deep ulceration and granulation tissue after which collagen deposition and contraction occur. If there is circumferential injury, a stricture may develop. Third-degree injuries are transmural with deep ulcerations that result in a black appearance to the lining of the esophagus. These injuries can result in esophageal perforation. Patients with grade 2b or 3 will develop strictures in 70–100% of cases.27,28 Endoscopic grading of mucosal injury directly predicts risk of complications with a ninefold increase in morbidity with each incremental increase in injury grade.29 Patients who present with peritonitis, mediastinitis, disseminated intravascular coagulation, or shock may require emergency resection of the damaged esophageal tissue.
TABLE 26-1
Classification of Caustic Esophageal Injuries
| Grade | Endoscopic Findings |
| 1 | Mucosal edema and erythema |
| 2a | Friability, hemorrhage, blisters, erosions, erythema, white exudate |
| 2b | Findings of grade 2a plus deep or circumferential ulceration |
| 3a | Small and scattered area of necrosis |
| 3b | Extensive necrosis |
Following a corrosive ingestion, patients may be asymptomatic or may present with nausea, vomiting, dysphagia, odynophagia, drooling, abdominal pain, chest pain, or stridor. There are no conclusive data to correlate laboratory values or symptoms with degree of injury. The absence of symptoms or oropharyngeal lesions does not exclude esophageal injury. In fact, 12% of patients who are asymptomatic and 61% of patients without oral injury will be found to have esophageal injury at endoscopy.26,30,31 In symptomatic patients, the presence of three or more symptoms is an important predictor of severe esophageal injury.28
There is some controversy regarding whether all patients with a history of corrosive ingestion need to undergo endoscopy. Some authors advocate that all patients with suspected corrosive ingestion undergo endoscopy as part of the medical evaluation because even asymptomatic patients may have esophageal injury.27,32 However, these injuries are typically mild, require no further acute treatment, and are at low risk for long-term complications. There is some evidence that asymptomatic patients may not benefit from routine endoscopy.28,33 Certainly all patients who are symptomatic require endoscopic evaluation of the esophagus.
Patients found to have grade 1 or 2a injury on endoscopy can be allowed oral intake and are discharged once symptoms have resolved. Patients with grade 2b and 3 injuries should be observed for 24 to 48 hours and then may have their diets slowly advanced. Because of the frequency with which strictures occur in grades 2b and 3 injuries, these patients should have a barium swallow on day 21 after injury to evaluate for stricture (Fig. 26-2). Once a stricture is identified, gradual dilations are initiated. Strictures refractory to dilation may need operative resection.

FIGURE 26-2 This barium swallow was performed three weeks after lye ingestion. Note the significant narrowing in the proximal two-thirds of the esophagus.
There is no standardized acute management protocol for caustic esophageal injuries. There are several authors who advocate the use of antibiotics, steroids, and proton pump inhibitors in the treatment of severe esophageal injury.27,31,32 Prospective studies have shown no benefit for the use of steroids in the treatment of caustic esophageal injuries in children.34 There have been no rigorous studies evaluating the use of antibiotics or proton pump inhibitors in these patients. Because of the heterogeneous nature of ingestions and the various substances, location, and degree of injury, the optimal management remains unclear.
Treatment modalities for esophageal strictures include bougienage, esophageal stent placement, intralesional corticosteroid injection, and endoscopic dilations after stricture formation. Multiple dilations may be required for strictures to resolve. Operative intervention may be necessary if these treatments fail, if malignant transformation occurs, or if lengthy or tight strictures develop. Esophageal carcinoma is a late but serious complication of severe caustic injuries. The incidence is 1000 times the expected occurrence rate of patients of a similar age.35 Long-term surveillance for development of esophageal malignancy in severe injuries is important.
Esophageal Strictures
In general, esophageal strictures in children do not involve malignancies. The causes of benign esophageal strictures in childhood include reflux esophagitis, corrosive ingestion, and anastomotic scarring. Anastomotic and corrosive strictures may be aggravated by GER. The incidence of stricture in patients with GER approaches 15%.36 Management includes relief of the obstruction as well as correction of the reflux. Anastomotic strictures tend to be discrete and short, whereas corrosive strictures are more likely to be irregular and long. Peptic esophageal strictures are short and usually located in the lower third of the esophagus (Fig. 26-3).

FIGURE 26-3 This barium study was performed in a child with dysphagia and pain. There is marked narrowing (arrow) of the distal esophagus secondary to gastroesophageal reflux and a peptic stricture.
Treatment of strictures includes medical therapy, bouginage, fundoplication, stricture resection, and interposition grafting. Most commonly, the initial treatment of strictures is balloon catheter dilation with aggressive medical management of the GER. The theoretical advantage of balloon dilation over bouginage is that the stricture is gradually dilated by uniform radial force whereas bouginage exerts an abrupt shearing force that may cause injury to the mucosa leading to further scarring and stricture. Patients may need several dilations over several months. The perforation rate with balloon dilation is less than 2%.37,38 Strategies to prevent perforation include choosing a balloon size that is not greater than the size of the patient’s esophagus, not overinflating the balloon, and gradually increasing the size of the balloon over several sessions for tight strictures.
GER-associated strictures are treated with a combination of preoperative dilations and antireflux procedures.39 Preoperative management includes proton pump inhibitors, maximal nutritional support, and optimization of respiratory status. Fundoplication is delayed until nutritional optimization is met, esophagitis has resolved, and the stricture has been dilated. Most patients undergo three to five dilations prior to fundoplication. Postoperative dilations are then performed until the stricture is resolved. Almost 90% of patients have complete resolution of the stricture and the associated GER with this management protocol.
Esophageal Perforation
Esophageal perforation is a rare but life-threatening event in children. Iatrogenic injuries, as a result of nasogastric tube placement, stricture dilations, and endotracheal intubation are the most common reasons found in infants and children. Due to the fact the esophagus lacks a serosal layer, a perforation allows bacteria and digestive enzymes to leak into the mediastinum. The surrounding loose areolar connective tissue is unable to contain the spread of infection and inflammation, and may lead to mediastinitis, empyema, abscess, and sepsis.40
Esophageal perforations may be iatrogenic, or result from ingestion of a foreign body, caustic substances, spontaneous, infectious, or traumatic. In the pediatric literature, nearly 80% of esophageal perforations are attributable to iatrogenic causes.41–43 In children, the most common cause of iatrogenic esophageal perforation is from stricture dilation. The most common location of perforation in children is the thoracic esophagus. Typically, a perforation in the upper thoracic esophagus will result in findings in the left thorax, whereas perforations in the distal thoracic esophagus will present with right-sided thoracic findings. This is in contrast to the neonate, where the pharyngoesophgeal junction is the most common site of perforation. This is likely due to the fact this region is the narrowest area of the esophagus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


