Chapter 105 The Epidemiology of Adolescent Health Problems
Health outcomes also vary. About 16 million women aged 15-19 yr old give birth annually, accounting for 10% of births worldwide. The average adolescent birthrate in low-income countries is 5-fold that of high-income countries. Complications from pregnancy and childbirth are the leading cause of death among adolescents in developing countries; death as an outcome of pregnancy is rare in developed countries. Perceptions of feeling healthy also vary greatly by country as shown in Figure 105-1; those who do not feel healthy increases proportionately with age.
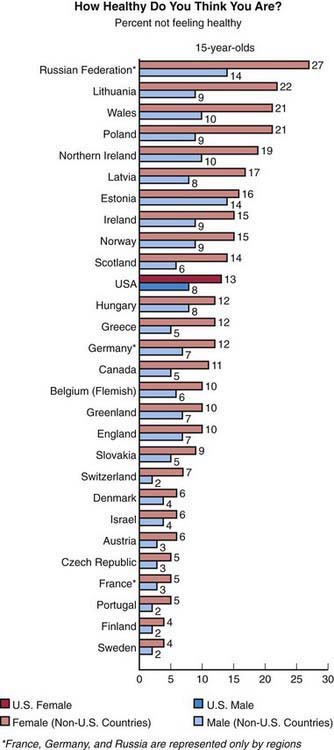
Figure 105-1 Proportion of 15 yr old youth from 28 nations who report not feeling healthy.
(From Health Resources and Services Administration, Maternal and Child Health Bureau: U.S. teens in our world. Understanding the health of U.S. youth in comparison to youth in other countries (website). www.mchb.hrsa.gov/mchirc/_pubs/us_teens/main_pages/ch_1.htm. Accessed April 16, 2010.)
Despite these variations by geographic region and level of economic development, there are many similarities in adolescent health issues. In all nations, adolescence is a time of immense biologic, psychologic, and social change (Chapter 104). Many of the psychologic changes have a biologic substrate in the development and eventual maturation of the central nervous system, particularly the frontal lobe areas responsible for executive functioning (Fig. 105-2). In addition to cognitive development, there are both risk and protective factors for adverse adolescent health behaviors that are dependent on the social environment as well as the mental health of an adolescent (Table 105-1).
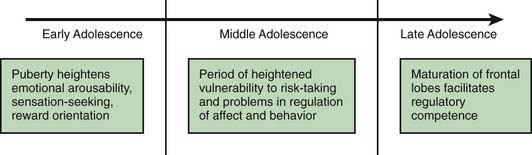
Table 105-1 IDENTIFIED RISK AND PROTECTIVE FACTORS FOR ADOLESCENT HEALTH BEHAVIORS
| BEHAVIOR | RISK FACTORS | PROTECTIVE FACTORS |
|---|---|---|
| Smoking | Depression and other mental health problems, alcohol use, disconnectedness from school or family, difficulty talking with parents, minority ethnicity, low school achievement, peer smoking | Family connectedness, perceived healthiness, higher parental expectations, low prevalence of smoking in school |
| Alcohol and drug misuse | Depression and other mental health problems, low self-esteem, easy family access to alcohol, working outside school, difficulty talking with parents, risk factors for transition from occasional to regular substance misuse (smoking, availability of substances, peer use, other risk behaviors) | Connectedness with school and family, religious affiliation |
| Teenage pregnancy | Deprivation, city residence, low educational expectations, lack of access to sexual health services, drug and alcohol use | Connectedness with school and family, religious affiliation |
| Sexually transmitted infections | Mental health problems, substance misuse | Connectedness with school and family, religious affiliation |
Adapted from Mclntosh N, Helms P, Smyth R, editors: Forfar and Arneil’s textbook of paediatrics,
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


