Chapter 101 The Endocrine System
The endocrinopathies are discussed in detail in Part XXVI.
Primary hypothyroidism occurs in approximately 1/4,000 births (Chapter 559). Because most infants with serious and treatable disease are asymptomatic at birth, all states screen for it. Thyroid deficiency may also be apparent at birth in genetically determined cretinism or in infants of mothers treated with antithyroid medications or during a pregnancy complicated by maternal hyperthyroidism. Constipation, prolonged jaundice, goiter, lethargy, or poor peripheral circulation as shown by persistently mottled skin or cold extremities should suggest cretinism. Early diagnosis and treatment of congenital thyroid hormone deficiency improve intellectual outcome and are facilitated by screening of all newborn infants for this deficiency.
Transient hypoparathyroidism may manifest as tetany of the newborn (Chapter 565).
Transient diabetes mellitus (Chapter 583) is rare and is encountered only in newborns. It usually manifests as dehydration, loss of weight, or acidosis in infants who are small for gestational age.
101.1 Infants of Diabetic Mothers
Pathophysiology
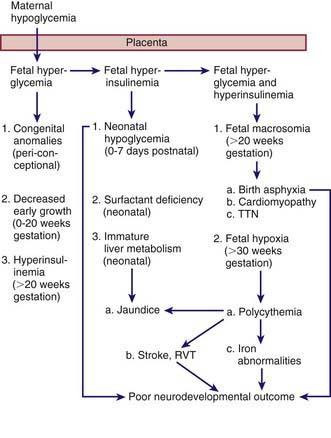
The probable pathogenic sequence is that maternal hyperglycemia causes fetal hyperglycemia, and the fetal pancreatic response leads to fetal hyperinsulinemia; fetal hyperinsulinemia and hyperglycemia then cause increased hepatic glucose uptake and glycogen synthesis, accelerated lipogenesis, and augmented protein synthesis (Fig. 101-1). Related pathologic findings are hypertrophy and hyperplasia of the pancreatic islet β cells, increased weight of the placenta and infant organs except for the brain, myocardial hypertrophy, increased amount of cytoplasm in liver cells, and extramedullary hematopoiesis. Hyperinsulinism and hyperglycemia produce fetal acidosis, which may result in an increased rate of stillbirth. Separation of the placenta at birth suddenly interrupts glucose infusion into the neonate without a proportional effect on the hyperinsulinism, and hypoglycemia and attenuated lipolysis develop during the first hours after birth.