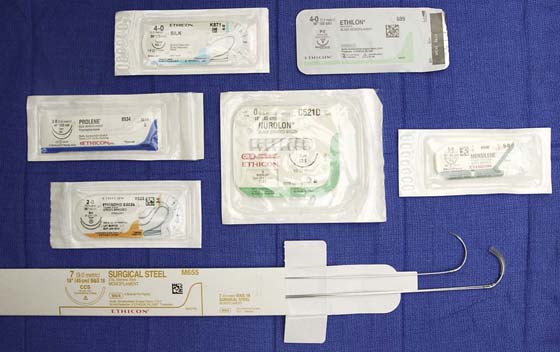
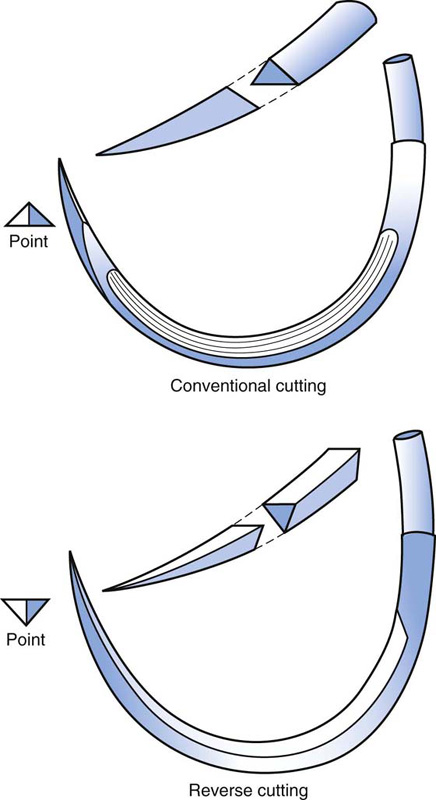
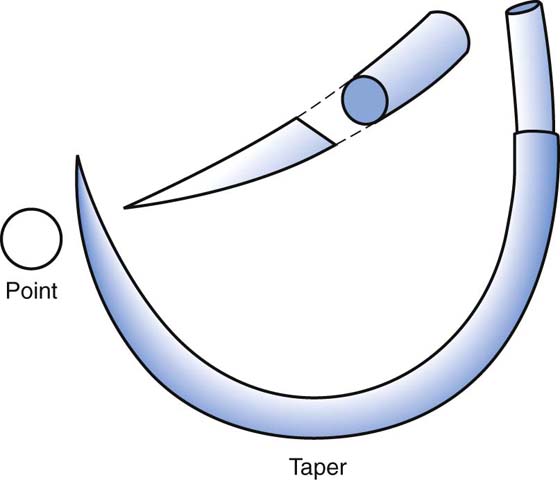
CHAPTER 4 Sutures are utilized to close wounds, to secure bleeding vessels, and to seal off visceral structures. A wide variety of suture materials are available, which vary in terms of size, material, content, and consistency. For purposes of explanation, sundry sutures can be divided into absorbable and nonabsorbable. Absorbable materials are broken down by the body’s enzyme systems and virtually disintegrate (Fig. 4–1). Nonabsorbable sutures resist enzymatic action and remain more or less permanently (with the exception of silk, which is gone within 2 years) in the body (Tables 4–1 and 4–2, Fig. 4–2). Tensile strength, particularly over time, is greater with nonabsorbable sutures. Sutures are sized on the basis of U.S. Pharmacopeia (USP)-equivalent diameters (Table 4–3). In infected tissues and otherwise dirty areas, absorbable sutures have an advantage in that they provide short-term tensile strength and then disappear. They are less likely to provide a foreign body nidus for continuous inflammation and infection, and for subsequent sinus formation. On the other hand, abdominal closure in the face of gross infection is an indication for the use of nonabsorbable suture material, to minimize the risk of dehiscence and/or evisceration. Almost all modern sutures are swaged onto a needle (Fig. 4–3). Needles generally may be divided into two overall groups: cutting and tapered. Cutting needles are used to penetrate denser and firmer tissues (e.g., fibrous tissue, periosteum, ligament fascia). Cutting needles have a triangular point (Fig. 4–4). If the additional cutting edge is on the inside curve of the needle, it is a standard cutting needle. If it is on the outside curvature of the needle, it is a reverse cutting needle. Tapered needles have a cone-shaped tip and are ideal for penetrating soft tissue and for producing the smallest hole (Fig. 4–5). A variety of needle configurations accompany the suture to which they are swaged. Straight needles are ideal for subcuticular closures. Very fine sutures (e.g., 5-0, 6-0) are usually equipped with ¼ or Suture should be selected on the basis of several parameters: (1) the volume of tissue to be secured, (2) the tensile strength of the tissue to be sutured, and (3) the potential for bacterial contamination. A general guideline that can guide a gynecologic surgeon recommends that the smallest suture that can adequately accomplish the work at hand is the best suture for the job. For example, to select a 0 or 1 suture to secure a small bleeding arteriole deep in the pelvis makes no sense when a 3-0 or 4-0 stitch would suffice. On the other hand, attempting to secure a uterine vessel pedicle or infundibulopelvic ligament pedicle with a 3-0 suture rather than a 0 suture is equally foolhardy. Braided suture has a greater propensity to become contaminated with debris and bacteria within the interstices of the braid compared with monofilament suture. Silk suture is easy to handle and easy to tie down, hence it forms a secure knot. It should never be used in the urinary bladder, and for that matter, neither should any nonabsorbable suture material. Nylon suture is very strong but requires many throws to avoid unraveling. Polyester suture material has all the advantages of silk and better strength and integrity. Polypropylene (Prolene) does not adhere to tissue and is less reactive than nylon. It is ideal for situations in which tissues are infected or contaminated. A very new structure concept has been developed by Covidien (New Haven, CT). The unidirectional barbed technology does not slip and does not require knot tying (Fig. 4–6B). FIGURE 4–1 A number of absorbable suture materials are illustrated: plain gut, chromic gut (top row), Vicryl (middle row), PDS, Maxon (bottom row). FIGURE 4–2 Nonabsorbable sutures include silk, monofilament nylon (top row), polypropylene, braided nylon, Mersilene, polyester (middle row), steel wire (bottom row). FIGURE 4–3 Several needle types are shown here with the suture material swaged to the needle. FIGURE 4–4 The top figure shows a standard cutting needle with triangular tip and cutting edge located on the inside curve of the needle. At bottom is a reverse cutting needle with the cutting edge positioned on the outer curve of the needle. FIGURE 4–5 The taper needle is seen to have a conical tip and creates a relatively smaller hole than does a cutting needle. FIGURE 4–6 A. This picture illustrates several varieties of circular needles. Top, a package containing a Several suture techniques are useful for pelvic surgery. The fascia or skin may be closed by simple interrupted sutures (Fig. 4–7A) or alternatively by mattress sutures (Fig. 4–7B, C). Subcuticular skin closures are commonly utilized for transverse abdominal incisions and for episiotomy closures (Fig. 4–8A, B). Alternatively, skin, subcutaneous tissue, and peritoneum may be closed by a continuous running suture (Fig. 4–8C). Visceral peritoneum is usually closed by a continuous running suture (Fig. 4–9). Bladder lacerations are typically closed with a continuous through-and-through chromic suture (Fig. 4–10). Fascia may be closed securely with a running monofilament suture of PDS, or polypropylene (Prolene) (Fig. 4–11). In critical circumstances, stainless steel wire, nylon, or Prolene may be utilized as interrupted sutures taken widely through the fascia and peritoneum en masse (Fig. 4–12). The Smead-Jones far-near technique may be utilized for patients at risk for dehiscence (Fig. 4–13A, B). Mass ligature techniques may be indicated with the use of #1 Prolene to repair eviscerated abdomens (Fig. 4–14). Vascular pedicles are secured by suture ligatures (Fig. 4–15A
Suture Material, Suturing Techniques, and Knot Tying
Suture Types
 circle needles. Intermediate sutures (e.g., 2-0, 3-0) usually have ½ to
circle needles. Intermediate sutures (e.g., 2-0, 3-0) usually have ½ to  circle needles. Large sutures most often have ½ circle needles (Fig. 4–6).
circle needles. Large sutures most often have ½ circle needles (Fig. 4–6).
Suture Selection
 circle. In the middle, a
circle. In the middle, a  circle and a ½ circle. Bottom, a ¼ circle and a
circle and a ½ circle. Bottom, a ¼ circle and a  circle. B. The V-Loc (polyglyconate) absorbable wound closure suture is barbed to prevent slippage and requires no terminal knot.
circle. B. The V-Loc (polyglyconate) absorbable wound closure suture is barbed to prevent slippage and requires no terminal knot.
Suture Techniques
![]()
Stay updated, free articles. Join our Telegram channel



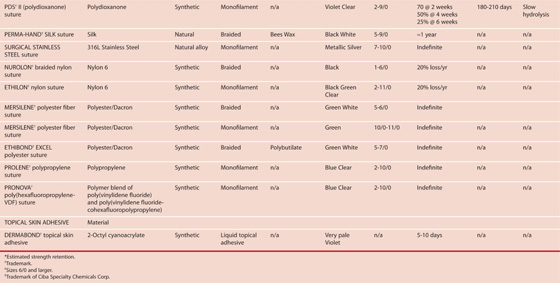
 Types of Suture Material
Types of Suture Material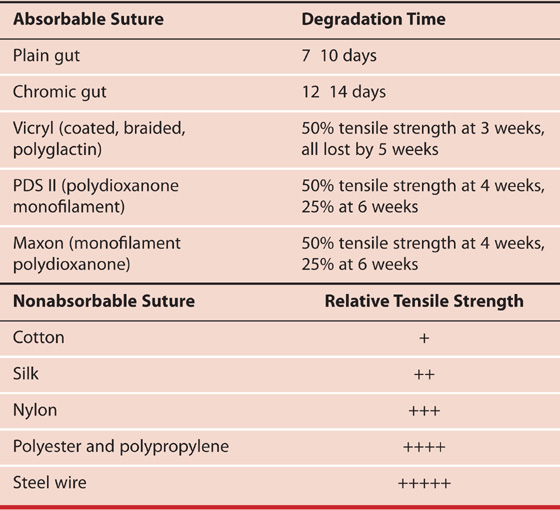
 Ethicon Suture Characteristics
Ethicon Suture Characteristics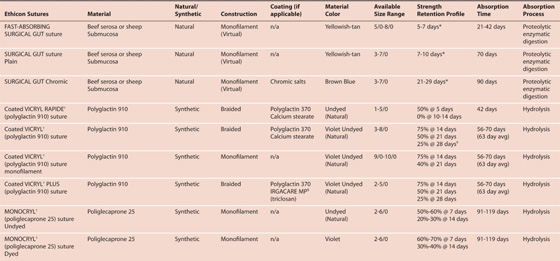
 Suture Size
Suture Size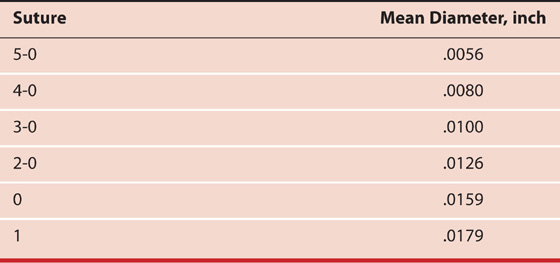

Full access? Get Clinical Tree


