11.5 Surgical conditions in the newborn
Oesophageal atresia
The diagnosis is confirmed by passing a large, firm catheter, for example a 10-French gauge orogastric tube, through the mouth and finding that it cannot be passed more than about 10 cm from the gums. The child must not be fed; otherwise, aspiration of feeds into the lungs is likely to occur. A plain X-ray of the torso will show gas in the bowel, confirming the presence of a distal tracheo-oesophageal fistula. About 50% of these infants have other congenital abnormalities, most of which form part of the VACTERL association (vertebral, anorectal, cardiac, renal and limb abnormalities; see Chapter 10.3). Major chromosomal abnormalities are seen in 5%, of which trisomy 18 and trisomy 21 are the most frequent. Many are premature and a history of maternal polyhydramnios is common.
Duodenal obstruction
Bile-stained vomiting starts soon after birth. The obstruction may be:
In duodenal atresia there may be other abnormalities, such as Down syndrome and imperforate anus (see Chapter 10.3). In the absence of birth asphyxia these infants are usually alert and feed well, but they vomit bile-stained material almost immediately. There may be epigastric distension. The diagnosis of duodenal atresia is made on plain X-ray of the abdomen, which reveals a characteristic ‘double bubble’ due to gas in the stomach and proximal duodenum (Fig. 11.5.1). Little or no gas will be visible distal to the obstruction. Duodenoduodenostomy is performed after resuscitation and correction of any fluid or electrolyte disturbance.
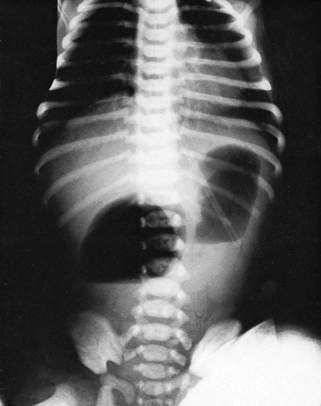
Distal bowel obstruction
In more distal bowel obstructions, vomiting remains a major feature but tends to occur later and is associated with abdominal distension. The more distal the obstruction, the later the vomiting and the more pronounced the distension (Fig. 11.5.2). The vomitus may become faeculent. An erect film of the abdomen will show distended loops of bowel and fluid levels (Fig. 11.5.3). The number of loops is dependent on the level of obstruction. The radiological appearances of Hirschsprung disease, meconium ileus and ileal atresia may be similar, and a contrast study, rectal biopsy or laparotomy may be required to make the definitive diagnosis.


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


