Background
Treatment of nonsevere hypertension during pregnancy is controversial. Sildenafil is a phosphodiesterase inhibitor that potentiates nitric oxide by promoting vasodilation. Nitric oxide plays a vital role in mediating the vascular adaptations during pregnancy.
Objective
The objective of the study was to determine whether treatment with sildenafil during pregnancy would lower maternal systolic blood pressure without adversely affecting fetal growth.
Study Design
Females with nonsevere hypertension (endothelial nitric oxide synthase +/– ) were cross-bred with normotensive wild-type males. At gestational day 1, pregnant dams were randomized to either sildenafil (0.4 mg/mL per day, comparable dose used in human pregnancy) or water for 3 weeks. Four groups were then generated: wild type (n = 7), wild type-sildenafil (n = 11), endothelial nitric oxide synthase +/– (n = 8), and endothelial nitric oxide synthase +/– sildenafil (n = 7). On gestational day 18, systolic blood pressure was measured. Dams were killed, fetal and placental weights were obtained, and carotid arteries were dissected to measure in vitro vascular reactivity with a wire-myography system. Responses to phenylephrine, L-NG-nitroarginine methyl ester, acetylcholine, and sodium nitroprusside were studied.
Results
Mean systolic blood pressure was elevated in the endothelial nitric oxide synthase +/– dams compared with wild-type controls ( P = .03). Treatment with sildenafil decreased systolic blood pressure in the endothelial nitric oxide synthase +/– –treated dams compared with nontreated endothelial nitric oxide synthase +/– dams ( P = .03). No differences were seen in the wild-type dams with or without sildenafil ( P = .47). Fetuses from endothelial nitric oxide synthase +/– dams were smaller compared with wild-type controls ( P < .001); however, when these endothelial nitric oxide synthase +/– dams were treated with sildenafil, fetal weight increased compared with the nontreated endothelial nitric oxide synthase +/– group ( P < .001). No difference were seen in wild-type groups treated or not treated with sildenafil ( P = .41). Placental weights were not significantly different among groups (endothelial nitric oxide synthase +/– sildenafil vs endothelial nitric oxide synthase +/– [ P = .48]; wild-type-sildenafil vs wild type [ P = .52]). Maximal vascular contraction induced by phenylephrine was blunted in endothelial nitric oxide synthase +/– dams treated with sildenafil compared with nontreated endothelial nitric oxide synthase +/– dams ( P < .01). No change in contractile response was seen in wild-type groups treated or not treated ( P = .53). When vessels were preincubated with L-NG-nitroarginine methyl ester, the contractile responses were similar among all groups ( P = .54). In addition, maximal vascular relaxation induced by acetylcholine was improved in the endothelial nitric oxide synthase +/– dams treated with sildenafil compared with endothelial nitric oxide synthase +/– nontreated dams ( P < .01). No change in relaxation response was seen in wild-type groups treated or not treated ( P = .62). Sodium nitroprusside did not change the contractile response in any of the groups ( P = .31).
Conclusion
Pregnant dams deficient in endothelial nitric oxide synthase, a nonsevere hypertensive murine model, treated with sildenafil had lower maternal systolic blood pressure, increased fetal growth, and improvement in vascular reactivity. Treatment with sildenafil may be beneficial in pregnancies complicated by nonsevere hypertension.
Nonsevere hypertension is clinically defined as a systolic blood pressure ranging from 140 to 170 mm Hg or a diastolic blood pressure ranging from 90 to 110 mm Hg. Although, nonsevere hypertension is a known risk factor for adverse pregnancy outcomes, treatment remains controversial. Use of antihypertensive therapy has been associated with maternal benefits such as a decrease in the frequency of severe hypertension and rate of antenatal hospitalization; however, it has also been associated with an increased risk of fetal growth restriction. Thus, there is a need for alternative antihypertensive therapies that improve pregnancy outcomes but minimize the perinatal risk.
The nitric oxide pathway is important in both hypertension and fetal growth restriction, playing a vital role in vascular adaptions during pregnancy. It is produced in the vasculature from the amino acid L-arginine by the enzyme endothelial nitric oxide synthase. Nitric oxide diffuses into vascular smooth muscle and stimulates the guanylate cyclase, which increases cyclic guanosine monophosphate to produce vasodilation. When cyclic guanosine monophosphate is broken down by phosphodiesterase, vasoconstriction occurs. Sildenafil, a phosphodiesterase inhibitor, can be given to block phosphodiesterase, preventing the degradation of cyclic guanosine monophosphate, resulting in vasodilation.
Using a murine model of nonsevere hypertension, we and others have previously shown that pregnant rodents deficient in endothelial nitric oxide synthase demonstrate a nonsevere hypertensive phenotype, fetal growth restriction, and altered vascular reactivity. There is evidence from ex vivo and animal models of growth restriction that the phosphodiesterase type 5 inhibitor, sildenafil, increases average pup birthweight and improves uteroplacental blood flow. Sildenafil may thus offer a potential therapeutic strategy to improve uteroplacental blood flow in human pregnancies complicated by hypertension. Therefore, our objective was to determine whether sildenafil treatment during pregnancy in a nonsevere hypertensive murine model will modulate maternal vascular reactivity to improve maternal blood pressure without reducing fetal growth.
Materials and Methods
Animals
The study protocol and procedures were approved by the institutional Animal Care and Use Committee of the University of Texas Health Science Center at Houston. Mature cycling female and male mice (4–6 weeks old) homozygous for the disruption of the endothelial nitric oxide synthase gene (endothelial nitric oxide synthase –/– , strain B6.129P2-Nos3tm1Unc, stock number 002684) and their age-matched wild-type controls (WT, strain C57BL/6J, stock no. 000664) were obtained from Jackson Laboratory (Bar Harbor, ME). The mice were housed separately in temperature-and humidity-controlled quarters with constant light/dark cycles of 12/12 hours. Mice were provided with food and water ad libitum. The same diet was used for all animals, including the offspring after they were weaned. Regular maintenance and care was provided by certified personnel and veterinary staff according to the guidelines of the Animal Care and Use Committee.
Male and female homozygous wild-type and endothelial nitric oxide synthase knockout (endothelial nitric oxide synthase –/– ) mice were bred to produce heterozygous (endothelial nitric oxide synthase +/– ) litters that developed in an abnormal uterine environment (maternal hypertension) to produce a nonsevere hypertensive phenotype as described in our previous publications ( Figure 1 A).
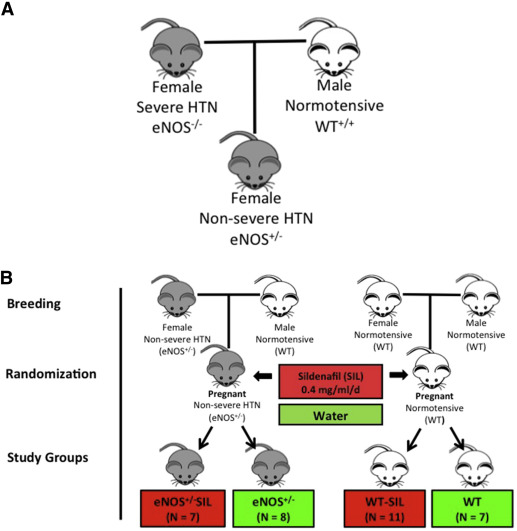
After 7–8 weeks of age, the endothelial nitric oxide synthase +/– dams with nonsevere hypertension were cross-bred with wild-type males. Gestational day 1 was defined by the presence of a sperm plug. Pregnant dams were randomly allocated to receive either water or sildenafil (SIL) dissolved in drinking water at 0.4 mg/kg per day from gestational day 1 to gestational day 18 (duration of the pregnancy). The dosage of sildenafil was based on the daily water consumption of pregnant mice and a review of prior mouse models utilizing sildenafil in pregnancy.
Four groups of pregnant dams were generated: wild type (n = 7), wild type -SIL (n = 11), endothelial nitric oxide synthase +/– (n = 8) and endothelial nitric oxide synthase +/– SIL (n = 7) ( Figure 1 B).
In vivo experiments
Water intake
Daily water intake was not different between wild-type treated with sildenafil vs water alone (wild type-sildenafil 5.1 ± 0.9 mL vs wild type 4.9 ± 0.7 mL; P = .31) or between endothelial nitric oxide synthase +/– treated with sildenafil versus water alone (endothelial nitric oxide synthase +/– sildenafil 4.8 ± 0.9 vs endothelial nitric oxide synthase +/– 5.0 ± 0.7 mL; P = .12).
Blood pressure
At gestational day 18 (term gestation), systolic blood pressure was measured using the noninvasive CODA tail cuff system (Kent Scientific). Animals were placed in a nose cone holder and onto a warming plate with the temperature preset at 37°C. A 17 mm tail cuff was applied to the base of the tail, and a pneumatic pulse transducer was then applied distal to the tail cuff. The tail cuff was programmed to insufflate to a maximal pressure of 250 mm Hg. A rest period of 15 seconds was allowed until the next insufflation. Mice underwent 10 acclimation cycles, followed by 20 cycles for data collection.
Fetal and placental weights
At gestational day 18, all pregnant dams were sacrificed by CO 2 inhalation per the Animal Care and Use Committee and the American Veterinary Medical Association guidelines. Fetal and placental weights were also obtained.
In vitro experiments
Vascular reactivity
Carotid arteries was dissected at the time of sacrifice on gestational day 18. Two millimeter segments (2–4 segments per animal) were mounted on a wire myograph (model 410A; J. P. Trading I/S, Aarhus, Denmark) using 25 μm tungsten wires. The arteries were bathed in physiologic salt solution that was maintained at 37°C with a pH of approximately 7.4. A mixture of 95% O 2 and 5% CO 2 was bubbled continuously through the solution. The force was recorded continuously by an isometric force transducer and analyzed with PowerLab data acquisition system and playback software (ADInstruments, Castle Hill, NSW, Australia).
Drugs and solutions
After stabilization of the tone, the arteries were contracted twice with 60 mmol/L KCl for 30 minutes to stabilize vascular responsiveness. The second contraction was used as the reference contraction in the final calculations. After 1 hour of equilibration in physiologic salt solution, contractile responses to the α 1 -adrenergic agonist phenylephrine (10 –10 to 10 –5 mol/L) were assessed in the presence and absence of a nonselective nitric oxide synthase antagonist (N-nitro-L-arginine methyl ester, 10 –4 mol/L).
In addition, relaxant responses to the endothelium-dependent acetylcholine (10 –10 to 10 –5 mol/L) were evaluated after precontraction of the arteries with phenylephrine to produce matching contractions in the 4 study groups. Finally, contractile responses to cumulative concentrations of sodium nitroprusside (10 –10 to 10 –5 mol/L) were studied in the presence and absence of N-nitro-L-arginine methyl ester ( Table 1 ).
| Agent | Type | Action | Dose, mol/L |
|---|---|---|---|
| Phenylephrine | α 1 -Adrenergic agonist | Smooth muscle contraction | 10 –10 to 10 –5 |
| L-NAME | Nitric oxide antagonist | Nonselective NOS inhibitor | 10 –10 to 10 –5 |
| Acetylcholine | Muscarinic agonist | Endothelium-dependent vasorelaxant | 10 –10 to 10 –5 |
| Sodium nitroprusside | Nitric oxide donor | Endothelium-independent vasorelaxant | 10 –10 to 10 –5 |
Agents were purchased from Sigma Chemical Co (St Louis, MO). After each agent was tested, vessels were washed with Krebs solution and left to recover for 30 minutes until they returned to their basal passive tension. The composition of Krebs solution was NaCl, 119 mmol/L; KCl, 4.7 mmol/L; NaH 2 PO 4 , 1.2 mmol/L; NaHCO 3 , 25 mmol/L; MgCl 2 , 1.2 mmol/L; CaCl 2 , 2.5 mmol/L; ethylenediaminetetraacetic acid, 0.026 mmol/L; glucose, 11.5 mmol/L.
Statistical analysis
Analysis was performed using SigmaPlot (Systat 11.0, Chicago, IL). Comparisons between groups were done using a 1-way ANOVA followed by a Neuman-Keuls multiple comparisons test. For vascular reactivity, the maximal effect of the dose response curve to each agent was calculated. Data are reported as mean ± SEM. A 2-tailed P < .05 was considered statistically significant.
Results
In vivo experiments
Maternal and litter weight
There was no difference in maternal weights at baseline or at term gestation (gestational day 18), average litter size, or total litter weight at birth between the 4 groups ( Table 2 ).
| Characteristics | WT (n = 7) | WT-SIL (n = 11) | eNOS +/– (n = 8) | eNOS +/– SIL (n = 7) |
|---|---|---|---|---|
| Maternal weight, g | 31.3 ± 1.3 | 30.5 ± 1.0 | 29.9 ± 1.1 | 30.5 ± 1.5 |
| Placental weight, g | 0.15 ± 0.02 | 0.16 ± 0.03 | 0.15 ± 0.01 | 0.17 ± 0.02 |
| Fetal weight, g | 0.84 ± 0.02 | 0.79 ± 0.07 | 0.70 ± 0.03 | 0.81 ± 0.02 |
| Litter weight, g | 5.8 ± 0.05 | 5.6 ± 0.11 | 4.4 ± 0.13 | 5.2 ± 0.03 |
| Litter size, n | 4.0 (2.0–6.0) | 5.0 (3.0–9.0) | 4.5 (3.0–6.8) | 5.0 (3.0–6.0) |
Maternal blood pressure
Mean systolic blood pressure was not different between wild-type groups (wild type vs wild type-sildenafil; P = .47). Mean systolic blood pressure was elevated in the endothelial nitric oxide synthase +/– dams relative to the wild-type control group as expected from our previous studies ( P = .03). Wild-type vs endothelial nitric oxide synthase +/– sildenafil was not significantly different ( P = .67) ( Figure 2 ).
Fetal weight
Fetal weight was not different between wild-type groups (wild type versus wild type-sildenafil; P = .41). Fetal weight was increased in the endothelial nitric oxide synthase +/– group treated with sildenafil (endothelial nitric oxide synthase +/– vs endothelial nitric oxide synthase +/– sildenafil; P < .001). Fetal weight was smaller in the endothelial nitric oxide synthase +/– group compared with the wild-type and wild-type-sildenafil groups; endothelial nitric oxide synthase +/– vs wild type and wild type-sildenafil were also significant ( P < .001). Fetal weights were not different in the wild-type vs endothelial nitric oxide synthase +/– sildenafil groups ( P = .54) ( Table 2 and Figure 3 ).
In vitro reactivity of the carotid arteries
Phenylephrine contraction and its maximal effect in carotid arteries from the pregnant dams were increased significantly in the endothelial nitric oxide synthase +/– group compared with the wild-type group ( P < .01). After the dams were treated with sildenafil, the contractile response of the carotid arteries from the endothelial nitric oxide synthase –/+ dams was blunted ( P < .01; Figure 4 A). No change was observed between the wild-type groups treated or not treated with sildenafil ( P = .53; Figure 4 B).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


