Severe Limb Shortening
Janice L. B. Byrne, MD
DIFFERENTIAL DIAGNOSIS
Common
Thanatophoric Dysplasia
Osteogenesis Imperfecta
Diabetic Embryopathy
Less Common
Achondrogenesis
Limb Reduction Defect
Rare but Important
Hypophosphatasia
Homozygous Achondroplasia
Amelia, Micromelia
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Is the shortening limited to a single bone, single limb, or generalized?
Are the long bones mildly shortened (1-3 standard deviations below the mean) or severely shortened?
Is the ossification normal?
Is the calvarium normally shaped?
Are there fractures?
Is there angulation or curvature of the long bones?
Are there other structural anomalies?
Is there a cystic hygroma or hydrops?
Helpful Clues for Common Diagnoses
Thanatophoric Dysplasia
Most common prenatally diagnosed lethal skeletal dysplasia
Polyhydramnios, often severe and progressive
Type I
Normally shaped calvarium
Micromelia
“Telephone receiver” femur
Normal ossification, without fractures
Platyspondyly
Small chest with short ribs
Trident hand
Other malformations rare
Type II
Cloverleaf-shaped calvarium (Kleeblattschädel)
Femora slightly longer and straighter than type I
Other features similar to type I
Osteogenesis Imperfecta
Multiple subtypes with most severe manifestations in perinatal lethal type II
Micromelia
Generalized decrease in ossification of all bones
Multiple fractures in utero
Ribs with “beaded” appearance due to fractures
Bones with irregular angulation due to fractures
Superb visualization of brain by ultrasound due to underossified calvarium
Diabetic Embryopathy
Uncontrolled diabetes is most common human teratogen
Femoral hypoplasia common manifestation of embryopathy
Shortening may be severe
Usually bilateral but may be asymmetrical
Preaxial polydactyly
Other structural anomalies involving central nervous system, heart, skeletal common
Caudal regression
More common in uncontrolled diabetes
Sacral agenesis with shortened legs in fixed, crossed leg “tailor’s posture”
Helpful Clues for Less Common Diagnoses
Achondrogenesis
Severe micromelia
Vertebral ossification absent
Small chest with short flared ribs, severe pulmonary hypoplasia
Disproportionately large head with normal or deficient ossification
Hydrops and cystic hygroma common in early gestation
Type IA most severely affected with unossified spine and skull, multiple rib fractures
Type IB without rib fractures
Type II with normal skull ossification but unossified spine
Limb Reduction Defect
May affect any segment of any limb
Usually single limb affected
Varying degrees of limb shortening
Longitudinal, intercalary and terminal transverse defects possible
Greatest shortening with transverse defects
May be seen with varicella exposure
Amniotic band related amputation may have similar appearance
Helpful Clues for Rare Diagnoses
Hypophosphatasia
3 main subtypes: Perinatal, infantile, adult onset
Perinatal onset associated with most severe limb shortening
Micromelia and hypomineralization, often severe, often lethal
Long bones thin and bowed
Calvarium may be severely underossified
Homozygous Achondroplasia
Autosomal dominant
Both parents must have achondroplasia
1/4 offspring with homozygous achondroplasia (lethal)
1/4 with average stature (unaffected)
1/2 with achondroplasia (heterozygous)
Limb shortening severe, onset in the mid-trimester
Chest is very small with associated pulmonary hypoplasia
Amelia, Micromelia
Amelia: Absence of 1 or more limbs
Tetra-amelia rare
Associated anomalies very common (cardiac, orofacial clefts, genitourinary)
High risk pulmonary hypoplasia, perinatal death
Micromelia: Shortening of both proximal and distal segments of limb
Association with severe, generalized syndromes
High risk perinatal lethality
Phocomelia: Shortening of limb with hand or foot arising near trunk
Other Essential Information
Most important approach in prenatal evaluation of short limbs is to determine lethal vs. non-lethal condition
Severity of limb shortening and chest size most informative
Severe limb shortening associated with evidence of a generalized chondrodystrophy usually lethal
Small chest correlated with risk of pulmonary hypoplasia
Severe polyhydramnios common in lethal conditions
Pattern of involvement is critical in formulating differential diagnosis
Are limb anomalies symmetric or asymmetric?
Are upper or lower limbs more severely affected?
Are the hands and feet present or absent; normal or abnormal?
Careful evaluation for other non-skeletal anomalies
Search for evidence of amniotic bands
Image Gallery
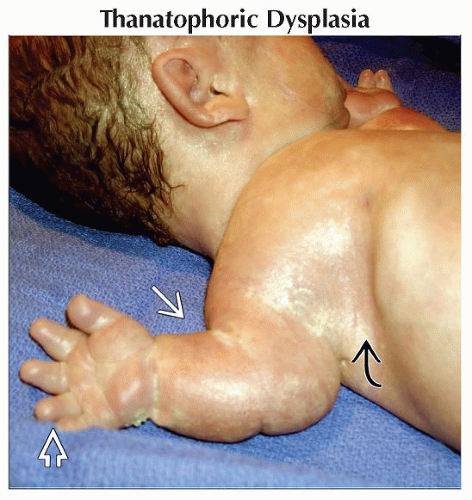 Clinical photograph shows a stillborn infant with thanatophoric dysplasia (TD). Micromelia  and a “trident” hand and a “trident” hand  are seen. The chest is bell-shaped are seen. The chest is bell-shaped  . . |
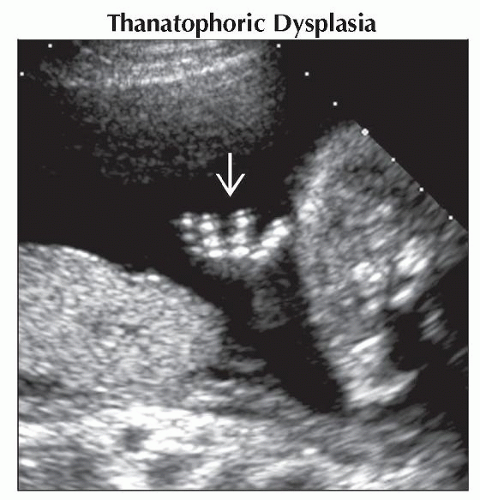 Coronal ultrasound shows a characteristic “trident” hand  of a fetus with thanatophoric dysplasia. of a fetus with thanatophoric dysplasia. |
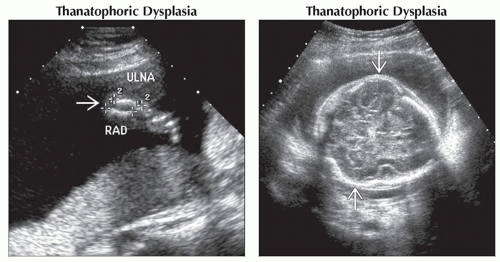 (Left) Ultrasound shows the very short radius and ulna
 in the forearm of a mid-trimester fetus with TD. (Right) Axial ultrasound shows the normally ossified calvarium of a mid-trimester fetus with TD. The parietal prominences in the forearm of a mid-trimester fetus with TD. (Right) Axial ultrasound shows the normally ossified calvarium of a mid-trimester fetus with TD. The parietal prominences  seen are characteristic of the “cloverleaf-shaped” skull seen in type II TD. seen are characteristic of the “cloverleaf-shaped” skull seen in type II TD.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|