Scrotal Mass
Sara M. O’Hara, MD, FAAP
DIFFERENTIAL DIAGNOSIS
Common
Inguinal-Scrotal Hernia
Epididymoorchitis
Hydrocele
Varicocele
Testicular Torsion
Torsion of Testicular Appendage
Testicular Rupture/Hematoma
Less Common
Spermatocele/Epididymal Cyst
Pyocele
Tubular Ectasia
Testicular Tumors
Rare but Important
Meconium Peritonitis
Scrotal Pneumatosis
Henoch-Schönlein Purpura
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Begin by determining structural origin of scrotal mass
Testicle
Epididymis
Tunica, surrounding testicle
Spermatic cord
Fat and connective tissues
Next, determine if mass is
Soft tissue
Cystic or fluid
Vascular
Peristalsing
Or mixture of these
Finally, confirm normal blood flow in testicle
Testicular ischemia can be complication of many scrotal masses
Helpful Clues for Common Diagnoses
Inguinal-Scrotal Hernia
Typically heterogeneous, mixed soft tissue mass
Look for hernia neck pointing to inguinal canal or frank communication with peritoneal cavity
Peristalsis may be diminished/absent when incarcerated
Testicle is usually displaced to bottom of scrotal sac
Epididymoorchitis
Enlarged, hypoechoic epididymis
May show increased echoes if there is hemorrhage
Marked hyperemia on Doppler
Associated hydrocele common
Hydrocele
Fluid within tunica
Surrounds testicle
Should not displace or compress testicle
Debris present with infection or trauma
Very common in baby boys
Varicocele
Dilated veins of pampiniform plexus
Left side > > right
Idiopathic type: Due to incompetent valves in internal spermatic vein
Secondary type: Due to increased pressure on draining veins
Most common correctable cause of male infertility
Varicoceles increase in size during Valsalva
Testicular Torsion
Twisting of testis and spermatic cord in scrotum
Spontaneous or traumatic
Results in ischemia/venous congestion
Surgical emergency
Testicular salvage rate drops with symptom duration
Doppler hypoperfusion is key to diagnosis
Always compare to asymptomatic side
Spontaneous detorsion, may appear hyperemic
Torsion of Testicular Appendage
Twisting of testicular or epididymal remnant
Hypoechoic mass adjacent to testis OR
Hyperechoic mass between testis and epididymis
Absent Doppler flow in mass with surrounding hyperemia
Associated hydrocele common
Typically less painful than testicular torsion
Testicular Rupture/Hematoma
Variable appearance depending on severity and acuity
Hematoma initially appears as echogenic avascular mass
Subsequently liquifies and contracts
Search testicular capsule for any breaks
Confirm testicular perfusion
Ruptured testicle is surgical emergency
Salvage rate drops with symptom duration
Extratesticular hematoma treated nonsurgically
Helpful Clues for Less Common Diagnoses
Spermatocele/Epididymal Cyst
Both result from dilated epididymal tubule
Spermatoceles
Contain spermatozoa and sediment
Most often in epididymal head
Epididymal cysts
Contain clear serous fluid
Found anywhere in epididymis
Pyocele
Infected collection
May be complication of prior trauma, surgery, bacteremia
Loculations and debris characteristic
Tubular Ectasia
Dilation of rete testis
Variably sized cysts or tubules
Radiate from mediastinum testis
No flow on Doppler
Testicular Tumors
Only 1-2% of all pediatric tumors
Bimodal age peaks
< 2 years old and young adults
Germ cell variety (60-77%)
Teratomas: Benign in pediatric patients (malignant in adults)
Yolk sac tumors: Elevated α-fetoprotein
Mixed: Variable behavior
Seminomas: Rare in children
Sertoli cell and Leydig cell tumors
Hormonally active: Gynecomastia, precocious puberty
Juvenile granulosa cell tumors
27% of all neonatal testicular tumors, benign
Gonadoblastoma: Intersex disorders
Leukemia/lymphoma secondary involvement, bilateral
Cystic dysplasia: Benign, associated ipsilateral renal agenesis/dysplasia
Extratesticular rhabdomyosarcoma
Highly aggressive malignancy
70% retroperitoneal nodal spread at diagnosis
Helpful Clues for Rare Diagnoses
Meconium Peritonitis
Extension into scrotum from peritoneum
Calcification common
Scrotal Pneumatosis
Extension from peritoneum or perineum
Benign or infectious varieties
Henoch-Schönlein Purpura
Marked swelling and hyperemia of peritesticular soft tissues
Usually bilateral
Testicles are normal
Image Gallery
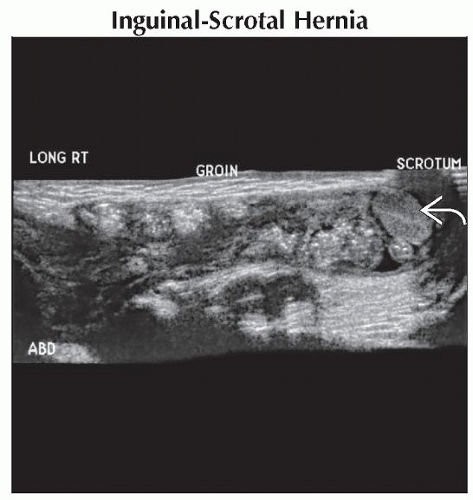 Longitudinal ultrasound with extended field of view shows bowel and fat extending through the inguinal canal into the scrotum in this child with scrotal fullness. The testicle  is displaced inferiorly. is displaced inferiorly. |
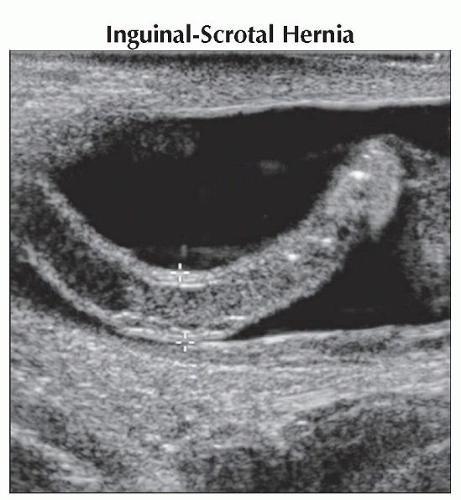 Transverse ultrasound shows the tubular appendix (calipers) extending into the right scrotal sac surrounded by fluid in this 2-month-old boy with scrotal swelling and pain.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|