I. Background
A. Description of the problem. School refusal is defined as “child-motivated refusal to attend school or difficulties remaining in school for an entire day.” It is a heterogenous, complex, and multicausal syndrome. Children with school refusal repeatedly stay home from school or are sent home from school for physical symptoms of emotional origin. School refusal is not a formal psychiatric diagnosis but, rather, a sign or symptom that leads to many possible diagnoses including social/school problems. Identified children and adolescents may suffer from significant emotional distress, especially anxiety and depression. Hersov described a common pattern of school refusal behavior that “often starts with vague complaints about school or reluctance to attend progressing to total refusal to go to school or to remain in school (Fig. 66-1) in the face of persuasion, entreaty, and punishment by parents and pressure from teachers, physicians, and education welfare officers.” The behavior may be accompanied by overt signs of anxiety or even panic when the time comes to go to school and although these children desire to attend school, many children cannot leave home to set out for school. The terms school refusal, school avoidance, and school phobia are often used interchangeably. School refusal is the preferred term because of its descriptive and comprehensive nature. Children with school refusal have different characteristics from children who are truant (Table 66-1). Truancy is defined as any unexcused, intentional, and unauthorized absence from compulsory schooling.
B. Epidemiology.
1. School refusal is the most common cause of vague physical symptoms in school-aged children. It is also the most common presentation of separation anxiety.
2. Approximately 5% of elementary school children and 2% of middle school children have this disorder. It is equally common in boys and girls.
3. It occurs across all socioeconomic groups.
4. School refusal has a bimodal peak: at 5-7 years of age and at 10-11 years of age.
5. The incidence of school refusal may be decreasing because of the increasing numbers of working mothers, which requires most children to master their separation fears long before entering kindergarten.
6. The homeschooling movement shelters many of these children.
C. Etiology. Many of these children have a shy and sensitive temperament. In general, affected youths are good to excellent students with no behavioral problems in the classroom. Approximately 20% of these children also have an acute precipitating event (e.g., being teased by someone at school).
1. Clinical studies have suggested three types of school refusers:
Separation-anxious school refusers. School refusal associated with separation anxiety disorder often begins following a period at home with a parent, such as a summer vacation, holiday break, or physical illness. It is more common in the younger children. Affects girls more than boys. Onset is usually seen when entering kindergarten. Mothers of these affected children were more likely to have experienced anxiety-based school refusal themselves compared with mothers of children who are phobic or anxious/depressed school refusers.
Phobic school refusers. These children have more severe and pervasive school refusal behavior. Later age of onset. Phobic stimuli include the school environment (school phobia), examinations, crowds, and animals
Anxious/depressed refusers. Often affect older children and adolescents. Affected adolescents frequently report moderate to severe somatic complaints of the autonomic (e.g., dizziness, diaphoresis, palpitations, shakiness) or gastrointestinal type (e.g., abdominal pain, nausea, diarrhea).
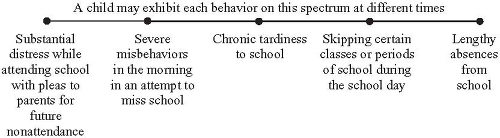
Figure 66-1. Spectrum of School Refusal Behavior.
2. Other causes.
a. Family functioning. Few studies have systematically evaluated and measured these problems. Family interactions that are associated with school refusal include the following:
Enmeshed parent-child dyads—characterized by dependency and overindulgence.
Conflictive families—characterized by high rates of coercion, noncompliance, and aggression.
Detached families—characterized by diffusion of activity and minimal intrafamilial interaction.
Isolated families—characterized by minimal extrafamilial contact.
Healthy families characterized by having an individual child with a behavioral problem. Most families of children with school refusal behavior show adaptive or healthy daily functioning.
b. Learning and language difficulties. This has not been extensively investigated. However, academic and communicative difficulties may have a significant contribution in the etiology of school refusal.
c. School-based stressors.
Environmental. May include-bathroom restrictions for children; unsupervised toilets, changing areas, and public areas causing the child to feel unsafe and vulnerable.
Academic. May include change of school or syllabus, excessive academic pressure, an impending test, a requirement to recite in class, a poor report card.
Interpersonal. May include discordant/adverse relationship with peers (e.g., bullying, teasing on the school grounds), loss of a school friend, teachers/supervisors unjustly blaming the child for their deficiencies, impersonal or hostile teacher-student relationships, physical fitness requirements for overweight or clumsy children.
Table 66-1. Criteria for differential diagnosis of school refusal and truancy
School refusal
Truancy
Severe emotional distress about attending school; may include anxiety, temper tantrums, depression, or somatic symptoms.
Lack of excessive anxiety or fear about attending school.
Parents are aware of absence; child often tries to persuade parents to allow him or her to stay home.
Child often attempts to conceal absence from parents.
Absence of significant antisocial behaviors such as juvenile delinquency.
Frequent antisocial behavior, including delinquent and disruptive acts (e.g., lying, stealing), often in the company of peers.
During school hours, child usually stays home because it is considered a safe and secure environment.
During school hours, child frequently does not stay home.
Child expresses willingness to do schoolwork and complies with completing work at home.
Lack of interest in schoolwork and unwillingness to conform to academic and behavior expectations.
Adapted from Fremont WP. School refusal in children and adolescents. Am Fam Physician 68(8):1555-1560, 2003.
Table 66-2. Presenting physical symptoms for school refusal
General—insomnia, excessive sleeping, fatigue, “always tired,” “fever,” “always sick” temper tantrums
Skin—pallor
Eye—blurred vision
ENT—recurrent sore throats, recurrent sinus problems, constant colds, dysphagia
Respiratory—hyperventilation, coughing tics, vocal cord dysfunction
Cardiovascular—palpitations,a chest painsa
Gastrointestinal—recurrent abdominal pains, anorexia, nausea, recurrent vomiting, diarrhea
Renal/genital—frequency-urgency syndrome
Skeletal—bone pain, joint pain, back pain, “fibromyalgia”
Neuromuscular—headaches,a dizziness,a syncope,a “weakness,” “always tired”
Pervasive symptoms—acute anxiety attack or panic reactiona
The symptoms are physiological manifestations of anxiety. The other symptoms may be fabricated or exaggerated.
a More common in older children.
D. Sequelae of school refusal. School refusal has very significant consequences.
Short-term consequences—poor academic performance, family difficulties and conflict, peer relationship problems, financial and legal consequences.
Long-term consequences—academic underachievement, fewer opportunities to attend institutions of higher education, employment difficulties, social difficulties, increased risk of psychiatric illness.
II. Making the diagnosis.
A. Signs and symptoms. Tables 66-2 and 66-3 review common presenting symptoms. Most children with school refusal complain of anxiety-related physical symptoms at the time of departure for school. When the child is permitted to stay home or is sent home from school, these symptoms quickly improve and completely disappear.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


School Refusal
School Refusal
Jan Harold D. Sia
Barton D. Schmitt
Carol C. Weitzman
