Rib Lesion
Christopher G. Anton, MD
DIFFERENTIAL DIAGNOSIS
Common
Normal Variant
Healing Rib Fracture
Less Common
Enchondroma
Osteochondroma
Metastasis
Osteomyelitis
Fibrous Dysplasia
Langerhans Cell Histiocytosis
Osteoblastoma
Rare but Important
Ewing Sarcoma
Aneurysmal Bone Cyst
Lymphoma/Leukemia
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
If palpable chest wall mass, image with chest radiograph 1st, ± rib radiographs
Asymmetric costochondral cartilage, congenital fused or bifid anterior rib
Many have characteristic diagnostic features and need no additional imaging
Helpful Clues for Common Diagnoses
Normal Variant
Bifid or fused ribs
Relatively common, up to 3% of population (supernumerary > agenesis/aplasia > errors of segmentation)
May present with firm or hard anterior chest wall mass
Chest radiograph is diagnostic
Healing Rib Fracture
Should be differentiated from pathologic fracture
If multiple posterior rib fractures, nonaccidental trauma should be excluded
Helpful Clues for Less Common Diagnoses
Enchondroma
Age: 15-40 years old
Lytic, well-defined with chondroid matrix, endosteal scalloping, marginal sclerosis, no periosteal reaction or soft tissue mass
Most commonly small tubular bones of hands and feet
Ollier disease
Nonhereditary
More common in boys
Multiple enchondromas
Mostly unilateral, predilection for appendicular skeleton
Sarcomatous transformation (5%)
Maffucci syndrome
Nonhereditary
Multiple enchondroma and soft tissue venous malformation
Unilateral involvement of hands and feet
Malignant transformation (15-25%)
Osteochondroma
Age: 10-25 years old
Most commonly around knee (35%)
Metaphysis of long bones (70%)
Pedunculated or sessile; grows away from joint
Multiple hereditary exostoses
Cartilage cap thickness is variable during childhood
Malignant degeneration
1% in solitary
3-5% in multiple hereditary exostoses
Should consider if rapid growth, indistinct lesion margin, osseous destruction, &/or soft tissue mass
Metastasis
Most commonly neuroblastoma
Lymphoma/leukemia
More commonly metastatic than primary involvement
Usually known malignancy
Osteomyelitis
Over 50% occur in preschool age children
Staphylococcus aureus most common pathogen for osteomyelitis in children (followed by Streptococcal pneumonia, Streptococcal pyogenes)
Most common pathogen in neonates
If more aggressive infection present, also consider actinomycosis (especially after dental procedures)
Aspiration of saliva
Pulmonary infiltrate/mass may spread to pleura, pericardium, chest wall
MRSA &/or ORSA becoming common cause of osteomyelitis
Chronic recurrent multifocal osteomyelitis (CRMO)
Unknown pathogen; not bacterial infection
Metaphyseal lesion but can occur anywhere
Pustulous dermatosis (psoriasis, acne, palmar or plantar pustulosis)
Pustulous dermatosis occurs in children/adolescents (25%) and adults (50%) with CRMO
Fibrous Dysplasia
Monostotic or polyostotic
Expansile, endosteal scalloping, lucent to ground-glass appearance
Sarcomatous degeneration in up to 0.5%
McCune-Albright: Female, precocious puberty, café au lait spots, and unilateral fibrous dysplasia
Langerhans Cell Histiocytosis
Flat bones (70%)
Monostotic (50-75%)
Well-defined or ill-defined margin, lytic ± sclerotic margin
Beveled edges in skull
Osteoblastoma
Benign osseous lesion with osteoid production
Age: 10-20 years old
> 1.5 cm (range 1-10 cm)
Most commonly located in posterior elements of spine
Expansile, lytic, cortex usually preserved ± internal calcification
May present with painful scoliosis
Helpful Clues for Rare Diagnoses
Ewing Sarcoma
Age: 10-25 years old
90% before age 20 years
Caucasians (96%)
Soft tissue or bone
Slight male predominance
Diaphysis of long bones (70%)
Ill-defined, lytic, permeative, moth-eaten, large, soft tissue mass; aggressive periosteal reaction (“onion skin,” “sunburst”)
Fever, leukocytosis, elevated ESR, soft tissue mass, localized pain
Other sarcomas
Ewing family of tumors, synovial cell sarcoma, chondrosarcoma, osteosarcoma, malignant peripheral nerve sheath tumor, primitive neuroectodermal tumor
Chest wall tumor ± rib involvement
Aneurysmal Bone Cyst
Expansile
Septated with fluid-fluid levels (CT or MR) ± periosteal reaction
Can present with pain and swelling
Often associated with other benign tumors
Lymphoma/Leukemia
Usually disseminated disease
Image Gallery
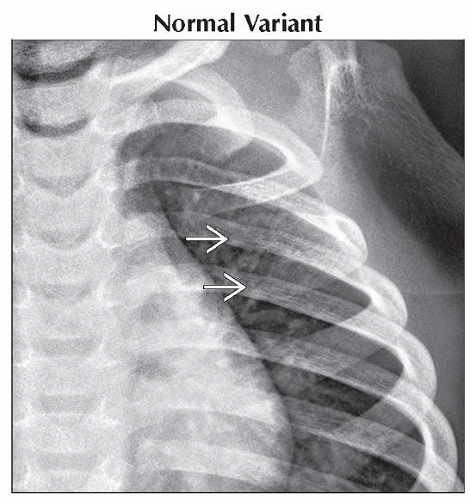 Anteroposterior radiograph shows an ill-defined, fork-shaped left anterior 3rd rib  . Rib anomalies are present in approximately 3% of the population. . Rib anomalies are present in approximately 3% of the population. |
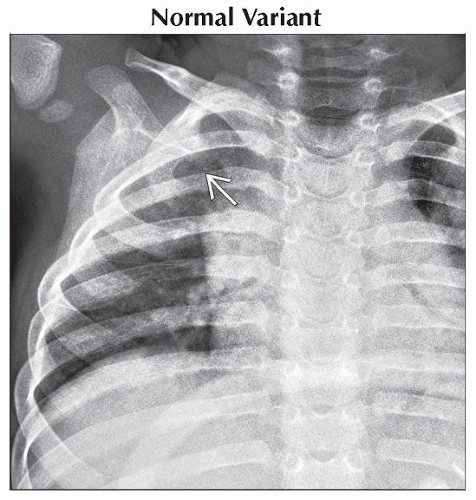 Anteroposterior radiograph shows congenital fusion
 of the anterior right 1st and 2nd ribs. In this young child, such fusion could present as a hard palpable supraclavicular mass. of the anterior right 1st and 2nd ribs. In this young child, such fusion could present as a hard palpable supraclavicular mass.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|