Chapter 374 Retropharyngeal Abscess, Lateral Pharyngeal (Parapharyngeal) Abscess, and Peritonsillar Cellulitis/Abscess
Retropharyngeal and Lateral Pharyngeal Abscess
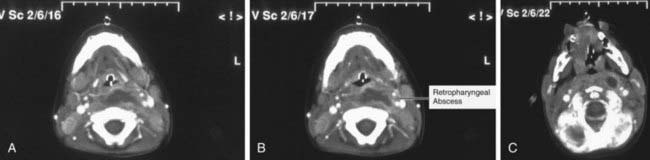
Incision for drainage and culture of an abscessed node provides the definitive diagnosis, but CT can be useful in identifying the presence of a retropharyngeal, lateral pharyngeal, or parapharyngeal abscess (Figs. 374-1 and 374-2). With CT scans, deep neck infections can be accurately identified and localized, but CT accurately identifies abscess formation in only 63% of patients. Soft tissue neck films taken during inspiration with the neck extended might show increased width or an air-fluid level in the retropharyngeal space. CT with contrast medium enhancement can reveal central lucency, ring enhancement, or scalloping of the walls of a lymph node. Scalloping of the abscess wall is thought to be a late finding and predicts abscess formation.