Remember that children who present with a neck mass have a number of considerations that can assist with the diagnosis, including location and associated findings
Michael S. Potter
Anthony Slonim MD
What to Do – Gather Appropriate Data
Several considerations need to be taken into account when a pediatric patient presents with a neck mass. Most neck masses in children are benign and due to either inflammation or congenital abnormalities, with 2% to 15% of persistent masses exhibiting malignancy. Figure 203.1 provides the three major categories for neck masses based upon age grouping.
In children, inflammation is the number one cause of neck masses. Lymphadenopathy is very common in children. However, 50% of children presenting with palpable lymph nodes of an appreciable size (1–1.5 cm) are not obviously infected or systematically ill. Children with cervical lymphadenopathy should be examined to determine a source for the adenopathy. Other variations of lymphadenopathy include lymphadenitis (acute and chronic) and suppurative lymphadenitis. Acute cervical lymph- adenitis is usually caused by regional viral infections such as rhinovirus or adenovirus. Similarly, chronic cervical lymphadenitis is also usually due to viral infections. When lymph nodes are unilateral or fluctuant, suppurative lymphadenitis caused by bacterial infections or common granulomatous diseases should be considered. The differential diagnosis includes Mycobacteria, cat-scratch disease, toxoplasmosis, actinomyces, but group A β-hemolytic streptococci and Staphylococcus aureus are often the primary causes. Salivary glands can also be the origin of neck masses: sialolithiasis, acute suppurative sialoadenitis, acute nonsuppurative sialoadenitis, or human immunodeficiency virus can all affect the salivary glands and cause neck masses.
Neck masses due to congenital conditions occur next in frequency after inflammation (Table 203.1). They are most easily classified by location either in the midline or lateral neck. Branchial cleft cysts and thyroglossal duct cysts are the most common congenital neck masses. Branchial cleft cysts, which occur in the lateral neck regions, typically present in childhood or early adulthood as nontender masses that become inflamed in the
presence of an upper respiratory tract infection. Lymphangiomas are also common lateral neck masses that typically present during a child’s first year of life. Thyroglossal duct cysts, occurring in the midline neck area, typically present as a midline neck mass that is asymptomatic. As with branchial cleft cysts, thyroglossal duct cysts can become infected. Other congenital neck masses include vascular anomalies, teratomas, and dermoid cysts. Vascular anomalies are typically noted at birth and can result in disfiguring and local compressive symptoms. Teratomas and dermoid cysts are usually painless masses that always occur in the neck’s midline.
presence of an upper respiratory tract infection. Lymphangiomas are also common lateral neck masses that typically present during a child’s first year of life. Thyroglossal duct cysts, occurring in the midline neck area, typically present as a midline neck mass that is asymptomatic. As with branchial cleft cysts, thyroglossal duct cysts can become infected. Other congenital neck masses include vascular anomalies, teratomas, and dermoid cysts. Vascular anomalies are typically noted at birth and can result in disfiguring and local compressive symptoms. Teratomas and dermoid cysts are usually painless masses that always occur in the neck’s midline.
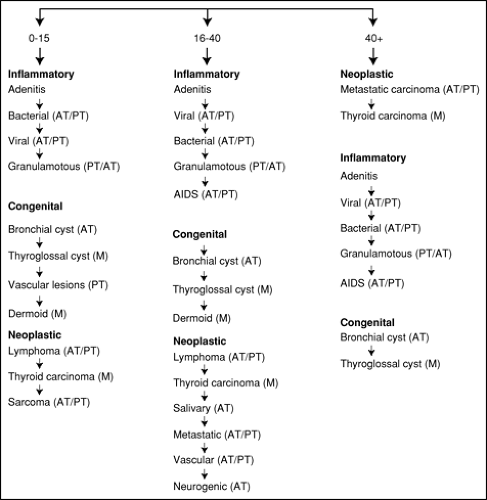 Figure 203.1. Relative frequency of specific neck masses within causative groups by age. AIDS, acquired immunodeficiency syndrome. Fedok FG, Burnett M. Evaluation of Neck Masses. In: Nobel J. Textbook of Primary Care Medicine. 3rd ed. St. Louis: Mosby, Inc.; 2001. |
Though infrequent in younger children, neoplastic neck masses can present in older children as painless, cervical masses that are fixed to the
deep cervical tissue, have grown quickly, or are located in the supraclavicular or posterior triangle areas of the neck (Table 203.1). Half of masses located in the posterior triangle area are malignant with half of those being Hodgkin lymphoma or non-Hodgkin lymphoma. Approximately 15% of these malignancies are due to neuroblastoma. Finally, thyroid tumors make up a significant percentage of malignant neck masses in children. Children who are younger than 6 years are most susceptible to neuroblastoma, non-Hodgkin lymphoma, rhabdomyosarcoma, and Hodgkin lymphoma, in that order of frequency. Children between the ages of 7 and 15 are equally likely to develop Hodgkin lymphoma or lymphosarcoma, followed by thyroid carcinoma, rhabdomyosarcoma, and parotid adenocarcinoma.
deep cervical tissue, have grown quickly, or are located in the supraclavicular or posterior triangle areas of the neck (Table 203.1). Half of masses located in the posterior triangle area are malignant with half of those being Hodgkin lymphoma or non-Hodgkin lymphoma. Approximately 15% of these malignancies are due to neuroblastoma. Finally, thyroid tumors make up a significant percentage of malignant neck masses in children. Children who are younger than 6 years are most susceptible to neuroblastoma, non-Hodgkin lymphoma, rhabdomyosarcoma, and Hodgkin lymphoma, in that order of frequency. Children between the ages of 7 and 15 are equally likely to develop Hodgkin lymphoma or lymphosarcoma, followed by thyroid carcinoma, rhabdomyosarcoma, and parotid adenocarcinoma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


