Pulmonary
Peter P. Moschovis
Lael M. Yonker
Elizabeth C. Parsons
Benjamin A. Nelson
Efraim Sadot
Christina V. Scirica
Kenan Haver
Natan Noviski
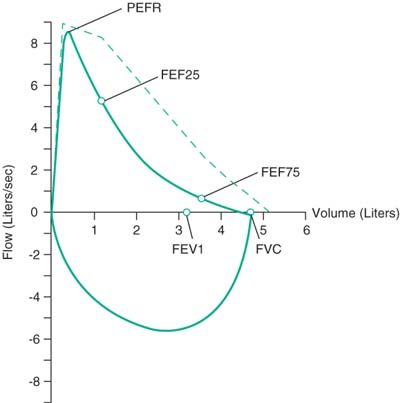
Pulmonary Function Tests
dImages: http://www.morgansci.com/customer-resource-center/pulmonary-info-for-patients/what-is-a-pft-test-2.php
Abbreviations
FVC: Max volume expired during forced expiratory maneuver
FEV1: Volume expired in 1st sec after max inspiration
FEV1/FVC: Measure of airflow obstruction
FEF25–75: Mid flow-rate of FVC (reflects small airways obstruction, less effort-dependent, but highly variable)
DLCO: Diffusion capacity of CO
PEFR: Peak expiratory flow rate
 |
 |
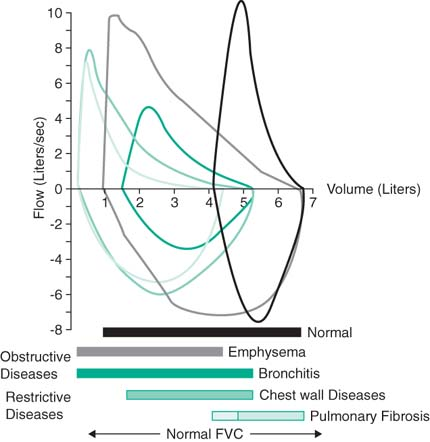
Obstructive lung disease: Asthma, protracted bronchitis, early cystic fibrosis
Restrictive lung disease: Thoracic (ILD, pneumothorax, edema, consolidation, fibrosis) and extrathoracic (obesity, resp muscle weakness, thoracic deformities, pleural disease)
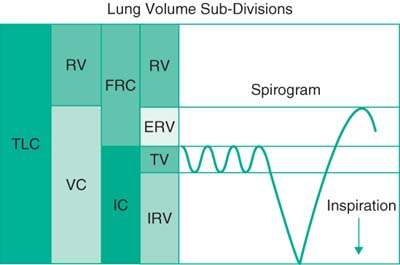
Basic Spirometry with Lung Volumes
Indications: Eval (1) if dysfxn, if obstructive, restrictive, or mixed & location & degree, (2) progression of known dz, (3) resp to bronchodilators
Relative contraindications: Hemoptysis of unknown origin, PTX, recent eye surgery (increased IOP during forced exp maneuvers)
| Parameter | Normal | Obstructive | Restrictive |
|---|---|---|---|
| FVC | ≥80% pred or LLN (Lower Limit Nml) | ↔↓ bronchodilator responsive: ↑12% or 0.2L | ↓↓ |
| FEV1 | ≥80% pred or LLN | ↓↓ bronchodilator responsive: ↑12% or 0.2L | ↔↓ |
| FEV1/FVC | 85% for 8–19 yo | ↓↓ | ↔↓ |
| RV | ↑ ↑ | ↓↓ (early) | |
| TLC | ↑ ↑ | ↓↓ (late) | |
| RV/TLC | ↑ ↑ | ↓↓ |
 |
Diffusion Capacity
Indications: Eval for parenchymal dz (DLCO measures “efficiency” of gas exchange)
DLCO dependent on TLC and Hgb; any process that ↓ them will ↓ DLCO as well
↓ DLCO can be 2/2: Parenchymal or pulm vascular dz, extrapulm restriction (lung resection, scoliosis), anemia (adjust for Hgb mathematically), tachycardia
Bronchial Provocation Testing
Indication: Suspect asthma, but spirometry normal
Procedure: Spirometry before/after progressive doses methacholine, histamine, exercise, mannitol, or hyperventilation/cold air
Positive test: FEV1 reduced 20% after challenge
Respiratory Muscle Strength
Indication: Rule out muscle weakness as a cause for respiratory insufficiency
Procedure: Pt breathes against shutter valve, measure max inspiratory pressure (MIP) and max expiratory pressure (MEP); perform at least 10× for consistency
Implications: Compare to age norms, MEP <50 cm H2O suggests insuff cough to clear secretions; MIP <-80 and MEP >+80 cm H2O r/o signif weakness (adults) Thorax 1984;39:535–538
Common Respiratory Complaints
Wheezing
Acute: Asthma, bronchiolitis, anaphylaxis, toxic inhalation, medication induced (β-blocker, ASA, indomethacin), aspiration
Chronic: Asthma, GERD, protracted bronchitis, asthma, CHF, vascular rings, tracheomalacia
Workup: Consider CXR if suspect asthma or aspiration, PFTs, pH probe, fluoroscopy for tracheomalacia or foreign body
Stridor
Inspiratory: Most common, extrathoracic origin
Laryngeal (most common): Laryngomalacia (most common chronic cause), croup (most common acute cause), laryngeal web/cyst, epiglottitis, vocal cord paralysis, subglottic stenosis (postintubation or congenital), foreign body, tumor (subglottic hemangioma or laryngeal papilloma), angioedema, traumatic intubation, laryngospasm (hypocalcemic tetany), psychogenic
Nasopharyngeal: Choanal atresia, lingual thyroid or thyroglossal cyst, macroglossia or micrognathia, hypertrophic tonsils/adenoids (h/o snoring), RP or peritonsillar abscess (drooling, “tripod”-ing)
Tracheal: Tracheomalacia, bacterial tracheitis, external compression (cystic hygroma), TEF (worsens w/feeds)
Expiratory: Less common, intrathoracic; mimics asthma, but tracheal/bronchial
Tracheomalacia, bronchomalacia, vascular rings, extrinsic compression, psych
Diagnostic clues:
Worse asleep → pharyngeal (tonsils, adenoids) origin
Worse awake/with agitation → laryngeal, tracheal or bronchial origin
Worse supine → laryngo/tracheomalacia, micrognathia, macroglossia
Acute: Infxn or foreign body; psychogenic (often w/o distress, neck flexed)
Workup: AP/lateral neck films to assess upper airway anatomy, chest film if suspect foreign body aspiration, direct bronch for persistent sx or foreign body, CT to r/o extrinsic compression, barium swallow to r/o vascular compression or GERD
Treatment: See ED section for acute treatment; treat underlying cause
Cough
Acute: URI, PNA, pneumonia, aspiration, PE
Chronic: Postnasal drip, GERD, bronchitis, TB, bronchiectasis, cough-variant asthma, toxic exposure (cigarette smoke), CHF, drug (ACE-I), ILD, BOOP
Workup: ENT exam for s/sx allergic rhinitis, CXR +/- sputum if suspect infection, CT scan if suspect BOOP or chronic ILD, empiric antacid if hx c/w GERD.
Laryngomalacia
Definition
(Pediatr Rev 2006;27:e33)
Floppy tissue above vocal cords that falls into airway w/ inspiration
Collapse of supraglottic structures (arytenoids cartilages and epiglottis) w/ inspiration
Epidemiology
Most common cause of stridor in infants (∼65%–75% of all cases)
Clinical Manifestations
Begins during first 2 mo of life; infant usually happy/thriving
Noises are inspiratory and may sound like nasal congestion
Exacerbated with crying, agitation, or during an upper respiratory infection
Prone position may diminish the stridor
Diagnostic Studies
History/physical, flexible laryngoscopy, and/or bronchoscopy
Prognosis
Self-limited condition, usually resolves w/o Rx by 12–18 mo of age
In 10% of affected pts, upper airway obstruct severe enough to cause apnea or FTT
When to Refer
FTT, feeding difficulty, respiratory distress/apnea/hoarseness, cyanosis, atypical clinical course/persistent stridor
Interventions
Surgery: Supraglottoplasty
Croup
Definition
Clinical dx for acute onset of barky cough, stridor, and respiratory distress.
Epidemiology
(N Engl J Med 2008;358:4:384)
Affects children btw 6 mo–3yr old. Incidence in boys is 1.5×’s > girls.
Seasonal: Peak Sept-Dec, biennial. 5% of 2 yo will develop croup.
Clinical Course
(Lancet 2008;371:329; N Engl J Med 2008;358:4:384)
Typically 12–48 hr of preceding URI sx’s, followed by acute barky cough, hoarse voice, and respiratory distress, which are worse at night. +/- fever, mild pharyngitis. 60% children have resolution of symptoms in 48 hr.
Microbiology
Parainfluenza 1, 3, influenza A, B, adenovirus, RSV, metapneumovirus
Diphtherial and measles rare causes in nonvaccinated children (Lancet 2008;371:329)
Pathophysiology
Subglottic edema and airway narrowing.
Differential Diagnosis
(Lancet 2008;371:329)
Epiglottitis: Dysphagia, anxiety, sniffing position, toxic appearing
Bacterial tracheitis: 2–7 d prodrome, febrile, toxic, do not respond to epi nebs
Foreign body aspiration: Sudden, no fever
Retropharyngeal/peritonsillar abscess: Dysphagia, drooling, neck stiffness, unilateral cervical lymphadenopathy
Angioneurotic edema: Urticarial rash
Allergic reaction: Urticarial rash, history of allergy
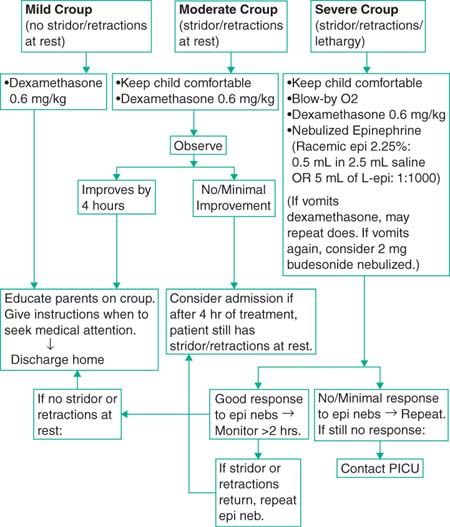
Treatment
(Lancet 2008;371:329; N Engl J Med 2008;358:4:384)
Keep child comfortable, leave in parent’s arms. Blow-by oxygen, often held by parent
Corticosteroids: Dexamethasone 0.6 mg/kg PO/IM ×1; duration of effect: 2–4 d
Racemic epinephrine: 0.5 mL of 2.25% racemic epi, or 5 mL of L-epi 1/1000
Improves symptoms within 10–30 min. Effect lasts 1–2 hr.
Heliox: For severe resp distress. Lower density helium, mixed w/ O2, ↓ turbulent flow through narrow airways. As good as, but more expensive than racemic epi.
No evidence that humidified air improves symptoms of croup. Antibiotics, antitussives, decongestants, or β2-agonists do not have a role in the Rx of croup.
Monitored at least 2–4 hr after racemic epi Rx before d/c, ensure no recurrence
Observation for 3–10 hr in ER following Rx reduces admission rate for croup.
 |
Obstructive Sleep Apnea Syndrome
(Arch Pediatr Adolesc Med 2005;159:775; Pediatrics 2002;109:704)
Definition
Breathing disorder during sleep w/ prolonged partial upper airway obstruct and/or intermittent complete obstruct (obstructive apnea); disrupts ventilation and sleep.
Needs to be distinguished from 1° snoring (PS), defined as snoring w/o obstructive apnea, frequent arousals from sleep, or gas exchange abnormalities.
Clinical Manifestations
Chronic snoring, daytime fatigue/sleepiness, sleep walking/talking, enuresis, periodic limb movement, headaches
Mouth breathing, nasal obstruct w/ wakefulness, adenoidal facies, hyponasal speech.
Neurocognitive deficits: Poor learning, behavioral problems, ADHD
Risk Factors
Adenotonsillar hypertrophy, obesity, craniofacial anomalies, neuromuscular d/o
Diagnosis
Pneumogram: Distinguishes between central and obstructive apnea
Polysomnography (PSG): Can distinguish PS from OSAS
Quantitative, noninvasive eval of frequency/severity of sleep disordered breathing
Confirm presence and severity of airflow obstruction; documents efficacy of Rx
Help determine the risk of postoperative complications
Determine the optimal level of CPAP when adenotonsillectomy is not an option
Studies have not determined which polysomnographic criteria predict morbidity
Treatment
Adenotonsillectomy: The most common treatment for children with OSAS
Resolution occurs in 75% to 100% after adenotonsillectomy
CPAP: Used indefinitely
For patients with specific surgical contraindications, minimal adenotonsillar tissue or persistent OSAS after adenotonsillectomy
Must be titrated in sleep lab before prescribing and needs periodic readjustment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


