Epidemiologic surveys have estimated that as many as 75% of women of reproductive age experience some symptoms attributable to the premenstrual phase of the menstrual cycle.1 More than 100 physical and psychological symptoms have been reported2; however, most women are able to manage these symptoms through lifestyle changes and conservative therapies. This phenomenon is often classified by the generic term premenstrual syndrome (PMS) and most often refers to any combination of symptoms that appears during the week prior to menstruation and that resolves within a week of onset of menses.3 Conversely, 3 to 8% of women of reproductive age report premenstrual symptoms of irritability, tension, dysphoria, and lability of mood, which seriously interfere with their lifestyle and relationships.4, 5, 6, 7, 8, 9, 10, 11 So disruptive is the latter that a series of research diagnostic criteria for what is now labeled premenstrual dysphoric disorder (PMDD) have been developed and published in the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (Table 8.1).12 Women who are found to meet the diagnostic criteria of PMDD do not usually respond to conservative and conventional interventions, and they often seek the expertise of a health professional.13
ETIOLOGY
The etiology of PMS, and specifically of PMDD, is still largely unknown. Attempts have been made to explain the phenomena in terms of biology, psychology, or psychosocial factors, but most of these explanations have failed to be confirmed by laboratory and treatment-based studies.
As is true for all female-specific mood disorders, the role of female sex hormones in PMDD has been considered of central importance. To date, however, studies attempting to attribute the disorder to an excess of estrogen, a deficit of progesterone, a withdrawal of estrogen, or changes in estrogen-to-progesterone ratio have been unable to find specific differences between women with PMDD and those without the disorder.14 Treatment studies have suggested that progesterone and progestogens may actually provoke rather than ameliorate the cyclical symptom changes of PMDD.15 The hypothesis that ovarian cyclicity is important in the etiology of PMDD is nevertheless supported by research. Efforts to suppress ovulation with estradiol patches and cyclical oral norethisterone, use of gonadotrophin-releasing hormone (GnRH) agonists, or bilateral oophorectomy resulted in the disappearance of premenstrual mood disturbances and physical symptoms.16, 17, 18
The current consensus seems to be that normal ovarian function (rather than hormone imbalance) is the cyclical trigger for PMDD-related biochemical events within the central nervous system and other target tissues. A psychoneuroendocrine mechanism triggered by the normal endocrine events of the ovarian cycle seems the most plausible explanation.19 This viewpoint is attractive in that it encourages investigation of the neuroendocrine-modulated central neurotransmitters and the role of hypothalamic-pituitary-gonadal (HPG) axis in PMDD. Data regarding the hypothalamic-pituitary-adrenal (HPA) axis function in women with PMS are conflicting. Overall, no differences between PMS patients and controls have been observed, but more recently, there is some indication that despite the ubiquity of affective symptoms in PMS, HPA axis function in PMS is distinctly different from that seen in major depression. Women with PMS fail to show the normal increase in HPA axis response to exercise and also seem to have a blunted adrenal sensitivity.20 They also appear to have an abnormal response to normal levels of progesterone,21 including physical evidence for an abnormal brain response to progesterone.22
Of all the neurotransmitters studied to date, increasing evidence suggests that serotonin may be important in the pathogenesis of PMDD.23, 24, 25, 26, 27 PMDD also shares many of the features of other mood and anxiety disorders linked to serotonergic dysfunction.28, 29, 30 In addition, reduction in brain serotonin neurotransmission is believed to lead to poor impulse control, depressed mood, irritability, and increased carbohydrate craving—all mood and behavioral symptoms associated with PMDD.31
Reciprocity between fluctuations in ovarian steroids and serotonergic function has been established in animals showing that estrogen and progesterone influence central serotonergic neuronal activity.32 In the hypothalamus, estrogen induces a diurnal fluctuation in serotonin,33 whereas progesterone increases the turnover rate of serotonin.34
TABLE 8.1 Summary of Premenstrual Dysphoric Disorder DSM-5 Criteria
A. In most menstrual cycles during the past year, five (or more) of the following symptoms occurred during the final week before the onset of menses, started to improve within a few days after the onset of menses, and were minimal or absent in the week postmenses, with at least one of the symptoms being either (1), (2), (3), or (4):
1. marked affective lability (e.g., mood swings; feeling suddenly sad or tearful or increased sensitivity to rejection)
2. marked irritability or anger or increased interpersonal conflicts
3. markedly depressed mood, feelings of hopelessness, or self-deprecating thoughts
4. marked anxiety, tension, feelings of being “keyed up” or “on edge”
6. subjective sense of difficulty in concentration
7. lethargy, easy fatigability, or marked lack of energy
8. marked change in appetite, overeating, or specific food cravings
9. hypersomnia or insomnia
10. a subjective sense of being overwhelmed or out of control
11. other physical symptoms such as breast tenderness or swelling, joint or muscle pain, a sensation of “bloating,” weight gain
B. The symptoms are associated with clinically significant distress or interference with work, school, usual social activities, or relationships with others (e.g., avoidance of social activities, decreased productivity and efficiency at work, school, or home).
C. The disturbance is not merely an exacerbation of the symptoms of another disorder, such as major depressive disorder, panic disorder, dysthymic disorder, or a personality disorder (although it may co-occur with any of these disorders).
D. Criteria A, B, and C should be confirmed by prospective daily ratings during at least two symptomatic cycles. (The diagnosis may be made provisionally prior to this confirmation.)
E. The symptoms are not due to the direct physiological effects of a substance (e.g., a drug of abuse, a medication, or other treatment) or a general medical condition (e.g., hyperthyroidism).
From American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorder. 5th ed. Washington, DC: American Psychiatric Association; 2013.
More recently, several studies concluded that serotonin function may also be altered in women with PMDD. Some studies used models of neuronal function (e.g., whole blood serotonin levels, platelet uptake of serotonin, platelet tritiated imipramine [Tofranil] binding) and found altered serotonin function during all phases of the menstrual cycle.23,35, 36, 37, 38 Other studies that used challenge tests (with L-tryptophan, fenfluramine [Pondimin], and buspirone [BuSpar]) suggested abnormal serotonin function in symptomatic women but differed in their findings as to whether the response to serotonin is blunted or heightened.25,39, 40, 41, 42 These studies imply, at least in part, a possible change in 5-hydroxytryptamine (serotonin) (5HT1A) receptor sensitivity in women with PMDD.
The current consensus is that women with PMDD may be behaviorally or biochemically subsensitive or supersensitive to biological challenges of the serotonergic system.43,44 It is not yet clear whether these women present with a trait or state marker of PMDD.
RISK FACTORS
Epidemiologic surveys from around the world continue to demonstrate convincingly that, for adult women, the lifetime prevalence of mood disorders is substantially higher than it is among men. Most studies confirm that the ratio of affected women to men is approximately 2:1, and this ratio is maintained across ethnic groups.45 The higher incidence of depression among women is primarily seen beginning at puberty and is less marked in the years after menopause.46 The relationship between PMDD and other psychiatric disorders is complicated by the observation that a high proportion of women presenting with PMDD have a history of previous episodes of mood disorders and that women with an ongoing mood disorder report premenstrual magnification of symptoms as well as an emergence of new symptoms.29,30,47, 48, 49, 50, 51, 52, 53 Likewise, several family studies have identified a concordance in rates of premenstrual tension between first-degree female family members.54, 55, 56 Women with PMS/PMDD also report more stressful life events,57 and more women with PMDD have histories of abuse (either sexual or physical) when compared with controls.58,59
PRESENTATION AND DIAGNOSIS
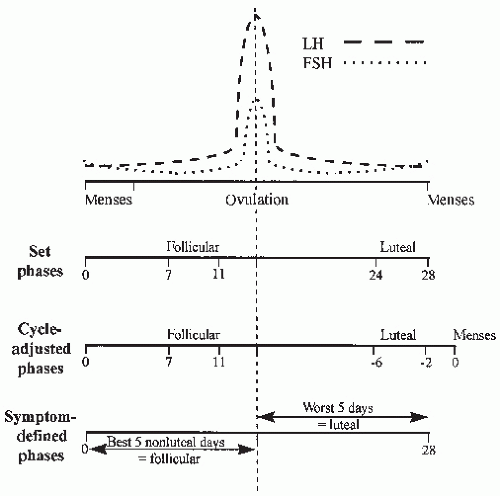
To aid in the study of menstrual cycle disorders, each menstrual cycle is characterized as containing two prominent phases: the follicular phase occurs after the onset of menses, and the luteal phase refers to the premenstrual interval. The temporal relationship between fluctuations in psychopathology and different phases of the menstrual cycle are well documented. It is therefore essential to ascertain whether the presenting premenstrual symptomatology is unique to the luteal phase or whether it is a worsening of an ongoing, persistent physical or psychiatric disorder.
Unfortunately, investigators have yet to reach consensus on how to best define the follicular and luteal phases of the menstrual cycle. Some investigators use set days, and others use cycle-adjusted days; other combinations also exist (Fig. 8.1). Although researchers are still defining the temporal boundaries of the follicular and luteal phases,60 a definition of the follicular phase as days 7 through 11 after onset of bleeding and the luteal phase as 6 days before bleeding through 2 days before bleeding seems most appropriate in clinical settings.
Another challenge in the delineation of premenstrual disorders is that most women report varying combinations of the most troubling symptoms. Some investigators attempted to divide the most prominent symptoms into physical and psychological domains; however, a complete separation is not possible. Measurement tools developed for depression and other mood disorders have not performed well in the diagnosis of PMS.61 A review by Budeiri et al.2 identified at least 65 instruments developed specifically to measure various combinations of premenstrual symptoms. Generally, if an instrument has been tested for reliability and validity in this population, it is appropriate for both facilitating diagnosis and assessing treatment outcomes. There has yet to be consensus as to which instruments are most appropriate for diagnosis and measurement of treatment efficacy,2,62 so most investigators use at least two or three of these instruments in their clinical trials.
FIGURE 8.1 The follicular and luteal phases can be defined in various ways for research purposes. The cycle-adjusted phases illustrated in the middle graph seem most appropriate to clinical settings. LH, luteinizing hormone; FSH, follicle-stimulating hormone.
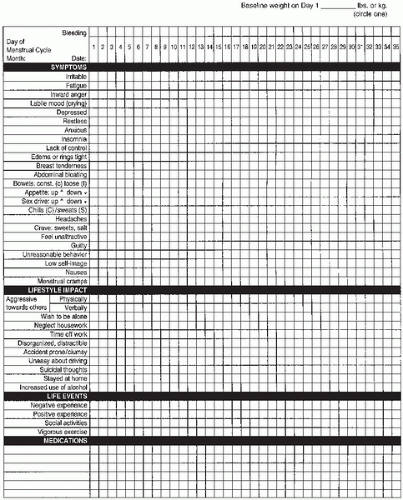
Women presenting with premenstrual complaints should be instructed to chart their symptoms daily over the course of several menstrual cycles to measure symptom change within each cycle. The current emphasis is on prospective self-report instruments, which are easy to administer and score without jeopardizing validity. The Daily Record of Severity of Problems (DRSP) assesses 20 symptoms associated with PMDD and specifically measures functional impairment in work and social realms.63 The Premenstrual Record of Impact and Severity of Menstruation (PRISM)64 and the Calendar of Premenstrual Experiences (COPE)65 are detailed one-page calendars that have also been validated and used in clinical trials. Figure 8.2 is a copy of the PRISM calendar, and Table 8.2 provides the instructions for completing it. These calendars allow respondents to rate a variety of physical and psychological symptoms, indicate negative and positive life events, record concurrent medications, and track menstrual bleeding and cycle length. Additionally, a premenstrual symptoms screening tool (PSST) has been developed that scores for both PMS and PMDD (Fig. 8.3).11
TABLE 8.2 Instructions for Completing the Premenstrual Record of Impact and Severity of Menstruation Calendar
Prepare the calendar on the first day of menstruation. Considering the first day of bleeding as day 1 of your menstrual cycle, enter the corresponding calendar date for each day in the space provided. Each evening, at about the same time, complete the calendar column for that day as described here:
• Bleeding:
Indicate if you have had bleeding by shading/filling in the box earlier that day’s date; for spotting, use an “X.”
• Symptoms:
If you do not experience any symptoms, leave the corresponding box blank. If present, indicate the severity by entering a number from 1 (mild) to 7 (severe).
• Lifestyle impact:
If the listed phrase applies to you that day, enter an “X.”
• Life events:
If you experienced one of these events that day, enter an “X.” Experiences: For positive (happy) or negative (sad/disappointing) experiences unrelated to your symptoms, specify the nature of the events on the back of the form. Social activities: This implies such events as a special dinner, show, or party, etc., involving family or friends. Vigorous exercise: This implies participation in a sporting event or exercise program lasting more than 30 minutes.
• Medication:
In the bottom five rows, list medication used, if any, and indicate days when medication was taken by entering an “X.”
From Reid RL. Premenstrual syndrome. Curr Probl Obstet Gynecol Fertil. 1985;8:1-57, with permission.
The lack of objective diagnostic tests for PMS or PMDD mandates taking a complete history of symptoms when one of these diagnoses is suspected. In addition to a history of the premenstrual symptoms, this interview should also include a complete review of physical systems (with particular attention to gynecologic and endocrine symptoms) and medical disorders, as well as a psychiatric history and a detailed review of family history looking for mental illness. Because the symptoms of anemia and thyroid disease often mirror those of PMS or PMDD, the patient should undergo laboratory studies if there is any hint of an underlying medical cause for the symptoms. In addition, women who are suspected to meet criteria for PMDD should be assessed by their physicians at least once during each cycle phase to ensure the patient subjectively endorses phase-appropriate mood symptoms that support their daily charting (minimal or no symptoms during follicular phase, lifestyleimpairing symptoms during the luteal phase).
The essential features of the DSM-5 PMDD criteria are the cyclicity of symptoms and the emphasis on core mood symptoms (criterion A), the requirement that the symptoms must interfere markedly with lifestyle (criterion B), and most important, the requirement that the disorder must be confirmed prospectively by daily ratings for at least two menstrual cycles (criterion D). Prospective daily rating of symptoms is now the only acceptable means of confirming a provisional DSM-5 diagnosis of PMDD.
FIGURE 8.2 The Premenstrual Record of Impact and Severity of Menstruation. Instructions for completing this calendar are provided in Table 8.2. (Reprinted from Reid RL. Premenstrual syndrome. Curr Probl Obstet Gynecol Fertil. 1985;8:1-57, with permission.)
The PRISM, COPE, DSR, and DRSP calendars contain the core symptoms and most of the additional symptoms considered for the DSM-5 diagnosis of PMDD. In using one of the daily calendars, the clinician must identify a priori the patient’s chief complaints and the symptoms to be followed throughout treatment. Daily symptoms are rated by the patient using scales that range from none (for a score of 0) to severe (for a score of 7 on the PRISM, 3 on the COPE). Scores for the symptoms of interest are added for the 5 follicular days and the 5 luteal days, and these total phase scores are then compared.
Investigators have typically followed a diagnostic severity criterion that is applied in addition to the criteria listed for PMDD in the DSM-5. Conventionally, an increase in symptom scores (worsening) of at least 30% from follicular to luteal phase scores within a single cycle is required to meet PMDD criteria.66 For inclusion of subjects in clinical trials, within-cycle worsening of at least 50% has been suggested.67 The within-cycle percent change is calculated by subtracting the follicular score from the luteal score, dividing by the luteal score, and multiplying by 100:
Only gold members can continue reading. Log In or Register to continue