(1)
Department of Obstetrics, Gynecology and Urological Sciences, University of Rome Sapienza – S. Andrea Hospital, Rome, Italy
Keywords
Septate uterusAFSHemi-uterusBicorporeal uterusHypoplastic uterusUterine malformations consist of a group of various congenital anomalies of the female genital system that have often been associated with increased miscarriage, preterm delivery and other adverse fetal outcome rates.
Uterine malformations are the result of four major disturbances in the development, formation or fusion of the Mullerian ducts during fetal life: (a) failure of one of the Mullerian ducts to develop (agenesis; AFS unicornuate uterus without rudimentary horn); (b) failure of the ducts to canalize; (c) failure or abnormal fusion of the ducts (AFS didelphys or bicornuate uterus); (d) failure of reabsorption of the midline uterine septum (AFS septate and arcuate uterus) [1].
Moreover, T-shaped uterus or hypoplastic uterus is a rare uterine malformation, except in woman exposed in utero to diethylstilbestrol (DES), an anti-abortive drug that used to be given to women with threatened miscarriage until the end of the Seventies [2]. The pathogenesis of this malformation remains unclear and its cause is still unknown.
The prevalence of congenital uterine anomalies in high-risk women is unclear as various diagnostic approaches have been applied to different groups of patients. In a recent, comprehensive systematic review Chan et al. [3] have identified 94 observational studies comprising 89,861 women. Pooled prevalence rates of uterine anomalies diagnosed by optimal tests are 5.5 % in the unselected population, 8.0 % in infertile women, 13.3 % in those with a miscarriage history and 24.5 % in those presenting miscarriage and infertility. That means that one out of four women with miscarriage and infertility harbor uterine anomalies.
Looking at the different classes of uterine anomalies, the so-called resorption or canalization defects, namely arcuate and septate uteri, have the highest prevalence rate (22.0 %) in high-risk patients with miscarriage and infertility, whereas unification defects have lower prevalence rates in the same patient population (bicornuate 4.7 %; unicornuate 3.1 %; Didelphys 2.1 %) [3].
The presence of a malformed uterus in a woman is thought to impair normal reproductive performance by increasing the incidence rates of early and late abortions, preterm deliveries and obstetrical complications. However, each uterine malformation may have a different effect on pregnancy outcome.
Hemi-uterus (AFS Unicornuate)
What is the probability for those patients to deliver a healthy child, and what specific obstetrics challenge will they face on the way to that desired endpoint? An investigation of the existing literature, largely anecdotal and incomplete, relies heavily on case reports and case series to prognosticate for these patients. However, women with untreated unicornuate uterus (hemi-uterus; Figs. 14.1, 14.2, 14.3) seem to have a relatively poor pregnancy outcome, even though a successful pregnancy is possible [4–12].


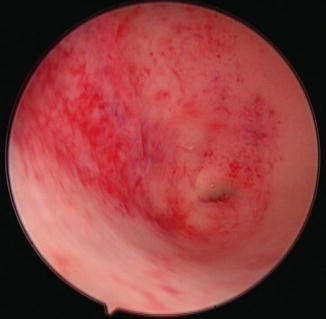
Fig. 14.1
3D ultrasound image of a hemi-uterus (ESHRE/ESGE Class U4)
Fig. 14.2
Hemi-uterus (ESHRE/ESGE Class U4) at hysterosalpingography (HSG)
Fig. 14.3
Hysteroscopic view of ahemi-uterus
The challenge faced by patients with unicornuate uterus has long been thought to be pregnancy maintenance rather than impaired fertility [5]. Patients with anomalies have higher frequencies of spontaneous abortions in the first and second trimester, preterm labor, and abnormal fetal presentations [6]. The assisted reproductive technology data, however, suggest that clinical pregnancy rates are reduced by 33 % in patients with unicornuate uterus, which contradicts the former statement [7].
Moreover, the rudimentary cavitated horn can be a site of implantation that results in horn gestation (ectopic pregnancy). This seems to be more likely in patients with AFS Class II a malformations (cavitated communicating horn) whose horn cavities are in direct communication with the primary uterine cavity. It is extremely uncommon to have an ectopic horn pregnancy in AFS Class Ib malformations, in which the rudimentary horn cavity does not communicate with the main uterine cavity, even though intra-abdominal sperm migration is a frequent occurrence in human reproduction [8]. Fedele et al. [9] have reported five cases of ruptured rudimentary horn containing ectopic pregnancy out of 49 patients with unicornuate uterus (10.2 %).
In this chapter, we cover mainly on data derived from the two most updated systematic reviews on that issue, In the first review, Grimbizis et al. [1] have assessed 151 patients pooled from 11 studies published between 1953 and the late 1990s. Out of a total of 260 pregnancies, the following rates are recorded: mean abortion, 37.1 %; mean preterm delivery, 16.4 %; mean term delivery, 45.3 (%); and mean live birth, 55.1 %.
The second and most updated report is by Reichman et al. [5] who have evaluated the data from 20 papers published up to 2006. In total, they have examined 290 women with unicornuate uterus, for an overall number of 468 pooled pregnancies. Overall, 2.7 % of pregnancies are ectopic, 24.3 % end in first-trimester abortion and 9.7 % in second-trimester abortion. The preterm delivery prevalence rate is 20.1 %, term deliveries account for 44.0 %. A very high rate of intrauterine fetal death is reported (10.5 %) as against a lower-than 50 % live-birth rate (49.6 %).
Therefore, the data reported in most recent studies are even worst when compared to the earlier ones, with high prevalence of ectopic pregnancies and fetal death in utero, and a live birth rate lower than 50 % (Table 14.1). If we look at the different subclasses of unicornuate uterus, we can see that subclass b (no rudimentary horn) is associated with the absolute lowest pregnancy outcome.
Table 14.1
Pregnancy outcome in patients with unicornuate uterus
Authors | Studies | Patients | Pregnancies | Ectopics | Abortions | Preterm del. | Term del. | Live birth |
|---|---|---|---|---|---|---|---|---|
N°. | N°. | N°. (%) | N°. (%) | N°. (%) | N°. (%) | N°. (%) | N°. (%) | |
Grimbizis et al. [1] | 11 | 151 | 260 | 3 (1.2) | 95 (36.5) | 42 (16.2) | 116 (44.6) | 141 (54.2) |
Reichman et al. [5] | 20 | 290 | 468 | 28 (6.0) | 114 (24.3)a | 86 (18.4) | 177 (37.8)b | 232 (49.6) |
Three main factors have been suggested as possible causes of such outcomes:
diminished muscle mass: the unicornuate uterus walls are thinner than normal, myometrium diminishes in thickness as gestational age advances, causing inconsistencies over different aspects of the uterus [5]. This reduced myometrial muscle thickness is supposed to play a role in both second-trimester abortion and premature delivery, which accounts for up to 25 % of these patients;
abnormal uterine blood flow: disturbance in the uterine blood flow caused by an absent or abnormal uterine or ovarian artery, which could explain growth restriction or spontaneous abortion. Poor vascularization could lead to impaired fetal nutrition, reduced fetal size and higher incidence of first-trimester abortion for compromised utero-placental blood flow [10];
cervical incompetence: even though, as reported by Reichman et al. [5], it seems unlikely that it plays a key role given that the great majority of pregnancy losses in unicornuate uteri occur during the first trimester.
Bicorporeal Uterus (AFS Bicornuate and Didelphys)
Bicornuate uterus, which is rare in the unselected population (0.4 %), is significantly more prevalent in women with infertility (1.1 %) and miscarriage (2.1 %), particularly if these coexist (4.7 %) [3].
Nevertheless, the relative frequency of having a bicornuate uterus in women presenting with a first-trimester recurrent pregnancy loss and a divided cavity seems to be very low as reported by some authors [13]. Maneschi et al. [14] has compared 13 patients with bicornuate uterus who had not undergone corrective surgery and 8 women treated with metroplasty, namely the Strassman procedure. The cumulative pregnancy rates are 67 and 95 % in patients without surgical repair and 63 and 88 % in the surgery-treated group. The probability of giving birth to a live-born infant is as follows: with no corrective surgery 30, 58 and 79 % for the first, second and third pregnancy, respectively; after corrective surgery 71 and 86 % for the first and second pregnancy, respectively.
Fertility seems not to be impaired in patients with bicornuate uterus, whereas gestational capacity is. A prognostic estimate of the likelihood of giving birth to a live-born baby can be formulated according to the number of pregnancies or surgical correction.
Based on the data reported in the literature on patients with untreated bicornuate uterus, even this malformation seems to have a poor pregnancy outcome. In the largest report published on the issue, out of 261 pooled patients from four studies with untreated bicornuate uterus for a total of 627 pregnancies, the mean abortion rate is 36.0 %, the mean preterm delivery rate 23.0 %, the mean term delivery rate 40.6 %, and the mean live-birth rate 55.2 %) [1].
In comparative studies on women with bicornuate uterus and normal controls, the pregnancy outcome in patients with bicornuate uterus is significantly poorer than that of patients with a normal uterus [15], whereas the miscarriage rate is significantly higher (41.8 % vs. 6.4 %; Risk ratio: 6.56) [16]. Even Shuiqing et al. [17] and Zlopasa et al. [18] have reported significantly high abortion rates in women with bicornuate uterus compared to controls (42.6 % vs. 9.1 %, risk ratio 4.69, and 27.5 % vs. 16.4 %, risk ratio 1.68, respectively).
Saravelos et al. [19] suggest that the miscarriage rate increases according to embryological severity of uterine anomalies. In 29 patients with bicornuate uterus they report a first-trimester miscarriage rate of 72.4 % (21/29) and a second-trimester miscarriage rate of 13.8 % (4/29) for a total miscarriage rate of 85.8 %. In this study, the pregnancy outcome in patients affected by bicornuate uterus seems to be really very poor, with a live birth rate of 13.8 %.
It is unclear if a complete bicornuate uterus has a poorer pregnancy outcome than partial bicornuate uterus since data in the literature are conflicting [15, 6].
As for Didelphys uterus, its prevalence is very low. According to Chan’s review [3] it is 0.1 % in the unselected population, 0.5 % in women affected by infertility, 0.5 % in women with miscarriage and 3.1 % in women with mixed infertility and miscarriage.
The pregnancy outcome in women with didelphys uterus seems to be similar to that of women with bicornuate uterus. A review of 152 pregnancies by 114 pooled patients with untreated didelphys uterus has revealed a mean 32.9 % abortion rate, a mean 28.9 % preterm delivery rate, a mean 36.2 % term delivery rate with a mean 56.6 % live birth rate [1].
Therefore, according to these data, didelphys and bicornuate uteri seem to have a similar effect on reproduction, since the presence of the second cervix and of the second channel seems not to have a beneficial effect, from a functional point of view, on the reproductive capability of the uterus.
Nevertheless, there are some conflicting data on that issue. Heinonen et al. [20], in the largest single series on women with didelphys uterus and pregnancy (49 cases), reported a mean miscarriage rate of 21 %, ectopic pregnancies in 2 %, prematurity in 24 %, fetal growth retardation in 11 % and perinatal mortality in 5.3 %. A fetal survival rate of 75 % has led the author to conclude that fertility in women with didelphys uterus is not impaired significantly, pregnancy prognosis is comparatively good, while prematurity and fetal growth retardation indicate meticulous prenatal care. Even Shuiqing et al. [17] has found a low incidence of first-trimester miscarriage rate in women with didelphys uterus as against women with normal uterus (9.5 % vs. 9.1 %, risk ratio 1.05). In our opinion, a possible explanation for this discrepancy could be seen in the difficulty that sometimes occurs in a correct diagnosis of the anomaly. Also, differential diagnosis between didelphys uterus and complete septate uterus with duplicatio cervix, being the latter an anomaly not included in most previous classification systems, could sometimes be an explanation for conflicting data.
Actually, the most salient difference between the two subtypes of unification defects remains the opportunity for a bicornuate uterus to be treated surgically, i.e. with laparotomic or laparoscopic Strassman metroplasty (Table 14.2) [21–25].
Table 14.2
Pregnancy outcome after Strassman metroplasty for bicornuate uterus
Authors | Patients | Pregnancies | Abortions | Live birth |
|---|---|---|---|---|
N°. | N°. | N°. (%) | N°. (%) | |
Candiani et al. [21] | 71 | 66 | 14 (19.7) | 52 (73.2) |
Maneschi et al. [22] | 8 | 7 | n.a. | 7 (88.0) |
Lolis et al. [24] | 22 | 19 | 0 (0) | 19 (86.4) |
Rechberger et al. [23] | 13a | 10 | 2 (16.6) | 8 (66.7) |
Total | 114 | 102 | 16 (14.1) | 86 (75.4) |
Occasionally, a bicornuate uterus is combined with the septum, and in most of those cases treatment does not vary from that of a septate uterus alone.
Septate Uterus
Canalization defects, namely subseptate or septate uteri, are significantly more common in women with miscarriage (5.3 %), especially if this is combined with a history of infertility (15.4 %) [3].
A septate uterus (Figs. 14.4, 14.5, 14.6) has generally been associated with the poorest reproductive performance, with fetal survival rates between 6 and 28 % and abortion rates up to 80 % [1]. The finding of a septate uterus per se is not a mandatory indication for surgery because it is not always associated with a severe reproductive performance [26, 27]. Ludmir et al. [28] have managed 42 patients with previously diagnosed but uncorrected uterine malformations: they have reported a 44 % pregnancy loss before the 25th week of gestation, 8 % premature deliveries, 48 % term deliveries and a fetal survival rate of 53 % in the septate group. Very similar to the latter are the data reported by Woelfer et al. [29]. in women with congenital anomalies detected incidentally by three-dimensional ultrasound. In this patient population considered at low risk of having an abnormal uterus, subseptate uterus is associated with first and second-trimester miscarriages in 45.6 % of cases and preterm labor in 10.5 % of cases. Nevertheless, the difference as against women with a normal uterus remains highly significant (Z =4.68).
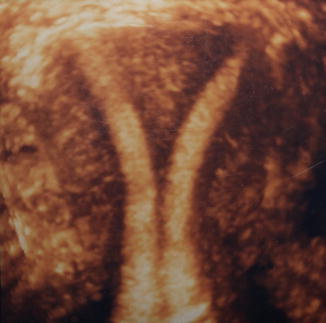
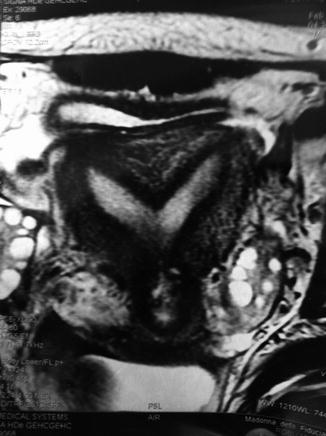

Fig. 14.4
3D ultrasound image of a complete septate uterus (ESHRE/ESGE Class U2b)
Fig. 14.5
MRI image of a partial septate uterus (ESHRE/ESGE Class U2a)
Fig. 14.6
Septate uterus (ESHRE/ESGE class U2) at hysteroscopy
In a survey on women with untreated septate uterus (four studies between 1982 and 1997, pooled patients/[1], the authors have reported a mean 44.1 % abortion rate, a mean 22.3 % preterm delivery rate, a mean 32.9 % term delivery rate and a mean 50 % live birth rate. These data suggest that pregnancy outcome in patients with untreated septate uterus remains significantly lower than in women with a normal uterus, even though not so low as reported in other studies [30], and it is close to that of women with an untreated bicornuate uterus.
Nevertheless, mention has to be made that the term ‘untreated’ means a woman who have not undergone/will not undergo corrective surgery, so that we could suppose it is the reproductive performance of a mixed group of patients with either asymptomatic and symptomatic infertility or miscarriage.
On the other hand, if we look at most studies concerning hysteroscopic metroplasty for septate uterus in women with infertility or miscarriage, the results are totally different from those reported in unselected untreated patients, with a very poor reproductive performance before surgery. In one systematic review [30] on 1,062 pooled pregnancies from 658 patients the miscarriage rate before hysteroscopic metroplasty is 88 %, preterm delivery rate is 9 %, and term deliveries rate is 3 %. In another review, [1] the data are very similar: out of 599 pooled pregnancies from 292 women the reported abortion rate is 86.4 %, preterm delivery rate is 9.8 %, term delivery rate 3.3 % and live birth rate only 6.1 %. Hence, we can suppose that in patients with a septate uterus who are symptomatic for infertility and/or miscarriage, wastage of the reproductive performance is an adverse reality.
Focusing on the most updated literature on the topic, we have found some remarkable studies published in the last 10 years, which supports the poor reproductive performance of selected patients with a septate uterus prior to hysteroscopic surgery. Gergolet et al. [31] has reported a miscarriage rate of 82.1 %, an ectopic pregnancy rate of 2.1 % and a live birth rate of 15.7 %; Saravelos et al. [32] have reached miscarriage, ectopic pregnancy and live-birth rates of 85.7, 4.7 and 9.4 %, respectively. Hollett-Caines et al. [33] and Pace et al. [34] have reported a nearly identical obstetrics history of their patients, with abortion and premature labor rates around 95 and 5 %. No data have been recorded on term delivery and live-birth rates, and we can presume it was nearly zero, as well as in the study by Venturoli et al. [35] who reported a 100 % abortion rate.
In conclusion, the review of the data seems to demonstrate a strong relationship between septate uterus and adverse reproductive outcome in selected patients with infertility and miscarriages.
Moreover, according to the systematic review and meta-analysis performed by Chan et al. [16], canalization defects (septate and subseptate uteri) are associated with reduced clinical pregnancy rates (R.R. 0.86) and increased rates of first-trimester miscarriage (R.R. 2.89), preterm birth (R.R. 2.14) and fetal malpresentation (R.R. 6.24).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


