CHAPTER 17 Practical application of electrodiagnostic studies to evaluate adult brachial plexus lesions
Summary box
Nerve conduction studies
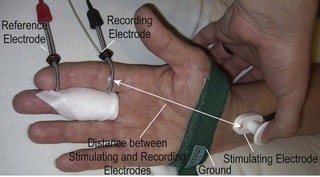
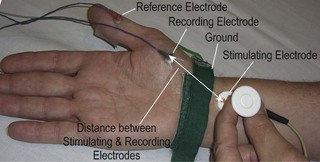
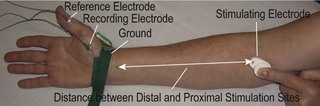
NCS evaluate both the motor and sensory fibers of a peripheral nerve; either a sensory nerve action potential (SNAP) or CMAP is recorded. Stimulating and recording techniques have been described for most of the major peripheral nerve branches in the upper extremity. Some techniques are facile and are reproducible from examiner to examiner; others are quite technically challenging to perform and not reliably reproducible. When performing NCS, body surface temperature of the extremity should be maintained at 32°C or higher, because cooling slows nerve conduction artificially, thereby affecting the recorded responses. Active and reference recording electrodes are placed over the course of the sensory nerve for sensory NCS (Figure 17.1). When studying motor nerve fibers, the active electrode is placed over the motor point of the muscle belly innervated by the relevant nerve, and the reference electrode is placed more distally over the muscle tendon (Figures 17.2, 17.3). For both motor and sensory NCS, the nerve is stimulated at a standard distance (which varies from one EDX laboratory to another) from the recording electrode; a grounding pad is placed on the skin between the stimulating and recording electrodes. The intensity and/or duration of the applied electrical stimulus is increased until a supramaximal response is achieved, indicating that all axons that can be stimulated have been stimulated. Amplitude and latency (time from onset of stimulus to initiation of the response) of the response are recorded.
Typically, both onset latency and peak latency of the sensory response (SNAP) are recorded (Figure 17.4). Onset latency is a reflection of the fastest conducting myelinated fibers, whereas peak latency is an approximation of the average conduction velocity of all the sensory fibers stimulated and recorded. Conduction velocity is directly proportional to diameter of the nerve fiber; therefore, the largest diameter myelinated fibers are the fastest. In sensory NCS, both the stimulus is applied and the response recorded directly from the same nerve; therefore, latency is a direct measure of the sensory conduction velocity, which can be calculated from latency and the distance between stimulation and recording sites. Sensory nerve conductions can be performed using either orthodromic (direction of physiologic nerve depolarization) or antidromic (opposite direction of normal depolarization) stimulation, which should provide similar results. Orthodromic sensory stimulation is more commonly used.
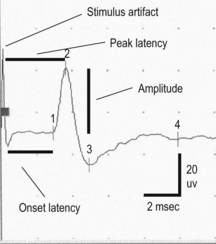
Figure 17.4 Normal median sensory-evoked response recorded from the index finger, as illustrated in Figure 17.1. Initial spike recorded at beginning of the tracing is the artifact generated with triggering of stimulus. Onset and peak latencies are measured in milliseconds and amplitude is measured in microvolts.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


